

Oval cell numbers in human chronic liver diseases are directly related to disease severity
- PMID: 10027411
- PMCID: PMC1849988
- DOI: 10.1016/S0002-9440(10)65299-6
Oval cell numbers in human chronic liver diseases are directly related to disease severity
Abstract
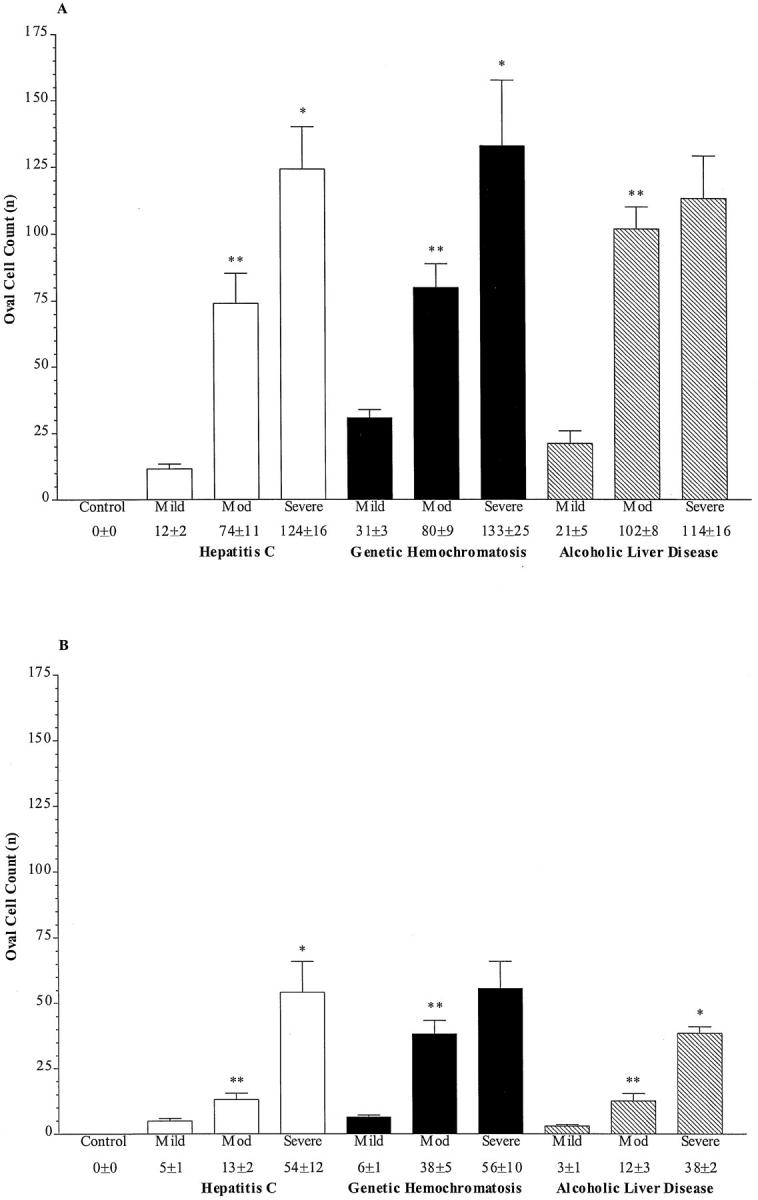
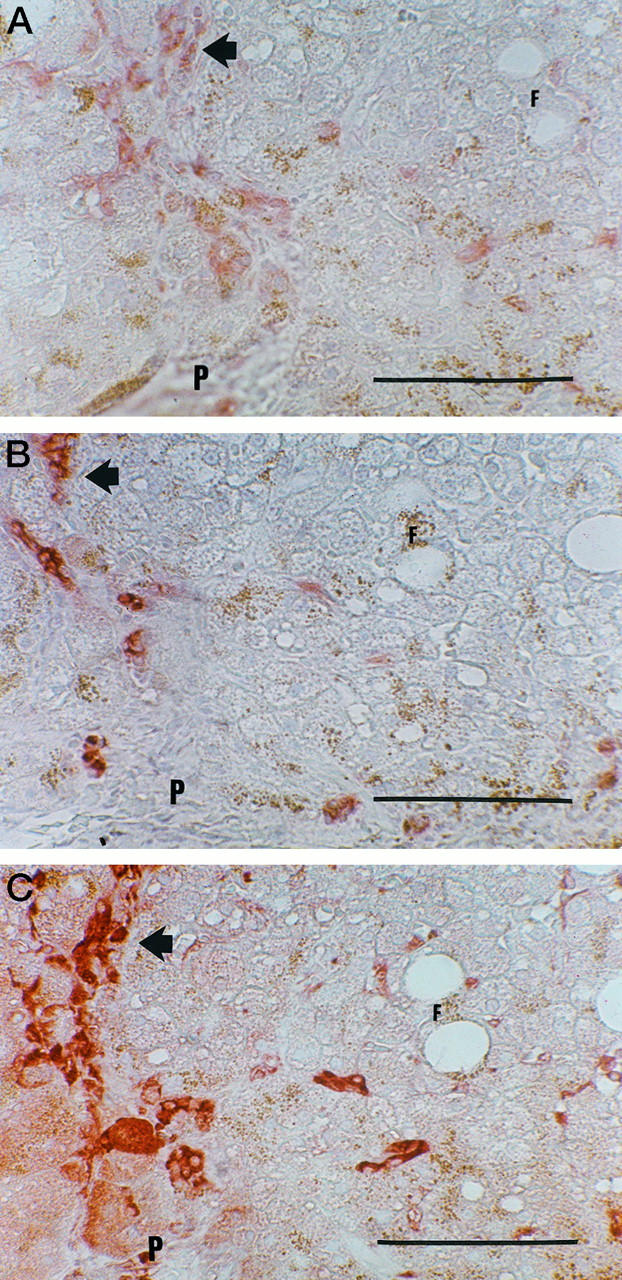
The risk of developing hepatocellular carcinoma is significantly increased in patients with genetic hemochromatosis, alcoholic liver disease, or chronic hepatitis C infection. The precise mechanisms underlying the development of hepatocellular carcinoma in these conditions are not well understood. Stem cells within the liver, termed oval cells, are involved in the pathogenesis of hepatocellular carcinoma in animal models and may be important in the development of hepatocellular carcinoma in human chronic liver diseases. The aims of this study were to determine whether oval cells could be detected in the liver of patients with genetic hemochromatosis, alcoholic liver disease, or chronic hepatitis C, and whether there is a relationship between the severity of the liver disease and the number of oval cells. Oval cells were detected using histology and immunohistochemistry in liver biopsies from patients with genetic hemochromatosis, alcoholic liver disease, or chronic hepatitis C. Oval cells were not observed in normal liver controls. Oval cell numbers increased significantly with the progression of disease severity from mild to severe in each of the diseases studied. We conclude that oval cells are frequently found in subjects with genetic hemochromatosis, alcoholic liver disease, or chronic hepatitis C. There is an association between severity of liver disease and increase in the number of oval cells consistent with the hypothesis that oval cell proliferation is associated with increased risk for development of hepatocellular carcinoma in chronic liver disease.
Figures

Similar articles
-
Hepatocyte proliferative activity in chronic liver damage as assessed by the monoclonal antibody MIB1 Ki67 in archival material: the role of etiology, disease activity, iron, and lipid peroxidation.Hepatology. 1996 Jun;23(6):1468-75. doi: 10.1053/jhep.1996.v23.pm0008675166. Hepatology. 1996. PMID: 8675166
-
Progenitor cell activation in chronic viralhepatitis.Liver Int. 2004 Jun;24(3):268-74. doi: 10.1111/j.1478-3231.2004.00908.x. Liver Int. 2004. PMID: 15189279
-
Hepatic oval cell response to the choline-deficient, ethionine supplemented model of murine liver injury is attenuated by the administration of a cyclo-oxygenase 2 inhibitor.Carcinogenesis. 2006 Aug;27(8):1607-16. doi: 10.1093/carcin/bgi365. Epub 2006 Feb 23. Carcinogenesis. 2006. PMID: 16497703
-
Steatosis as a cofactor in other liver diseases: hepatitis C virus, alcohol, hemochromatosis, and others.Clin Liver Dis. 2007 Feb;11(1):173-89, x. doi: 10.1016/j.cld.2007.02.007. Clin Liver Dis. 2007. PMID: 17544978 Review.
-
Iron and liver fibrosis: Mechanistic and clinical aspects.World J Gastroenterol. 2019 Feb 7;25(5):521-538. doi: 10.3748/wjg.v25.i5.521. World J Gastroenterol. 2019. PMID: 30774269 Free PMC article. Review.
Cited by
-
Improved Serum Alpha-Fetoprotein Levels after Iron Reduction Therapy in HCV Patients.ISRN Hepatol. 2014 Feb 4;2014:875140. doi: 10.1155/2014/875140. eCollection 2014. ISRN Hepatol. 2014. PMID: 27335844 Free PMC article.
-
Hepatic stem cells: from inside and outside the liver?Cell Prolif. 2004 Feb;37(1):1-21. doi: 10.1111/j.1365-2184.2004.00297.x. Cell Prolif. 2004. PMID: 14871234 Free PMC article. Review.
-
Towards Bioengineered Liver Stem Cell Transplantation Studies in a Preclinical Dog Model for Inherited Copper Toxicosis.Bioengineering (Basel). 2019 Sep 25;6(4):88. doi: 10.3390/bioengineering6040088. Bioengineering (Basel). 2019. PMID: 31557851 Free PMC article. Review.
-
Possible stem cell origin of human cholangiocarcinoma.World J Gastroenterol. 2004 Nov 15;10(22):3374-6. doi: 10.3748/wjg.v10.i22.3374. World J Gastroenterol. 2004. PMID: 15484322 Free PMC article.
-
Update on Hepatobiliary Plasticity.Semin Liver Dis. 2023 Feb;43(1):13-23. doi: 10.1055/s-0042-1760306. Epub 2023 Feb 10. Semin Liver Dis. 2023. PMID: 36764306 Free PMC article.
References
-
- Kew MC: Hepatic tumors and cysts. Feldman M Scharschmidt BF Sleisenger MH eds. Sleisenger and Fordtran’s gastrointestinal and liver diseases: pathophysiology/diagnosis/management. 1998, :pp 1364-1387 WB Saunders, Philadelphia
-
- Colombo M, Kuo G, Choo QL, Donato MF, Del Ninno E, Tommasini MA, Dioguardi N: Prevalence of antibodies to hepatitis C virus in Italian patients with hepatocellular carcinoma. Lancet 1989, 2:1006-1008 - PubMed
-
- Roudot-Thoraval F, Bastie A, Pawlotsky JM, Dhumeaux D: Epidemiological factors affecting the severity of hepatitis C virus-related liver disease: a French survey of 6,664 patients. The Study Group for the Prevalence and the Epidemiology of Hepatitis C Virus. Hepatology 1997, 26:485-490 - PubMed
-
- Tsukuma H, Hiyama T, Tanaka S, Nakao M, Yabuuchi T, Kitamura T, Nakanishi K, Fujimoto I, Inoue A, Yamazaki H, Kawashima T: Risk factors for hepatocellular carcinoma among patients with chronic liver disease. New Engl J Med 1993, 328:1797-1801 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
