

Results of three to 10 year follow up of balloon dilatation of the pulmonary valve
- PMID: 10065029
- PMCID: PMC1728864
- DOI: 10.1136/hrt.80.6.591
Results of three to 10 year follow up of balloon dilatation of the pulmonary valve
Abstract
Background: The results of immediate and short term follow up of balloon dilatation of the pulmonary valve have been well documented, but there is limited information on long term follow up.
Objective: To evaluate the results of three to 10 year follow up of balloon dilatation of the pulmonary valve in children and adolescents.
Setting: Tertiary care centre/university hospital.
Design: Retrospective study.
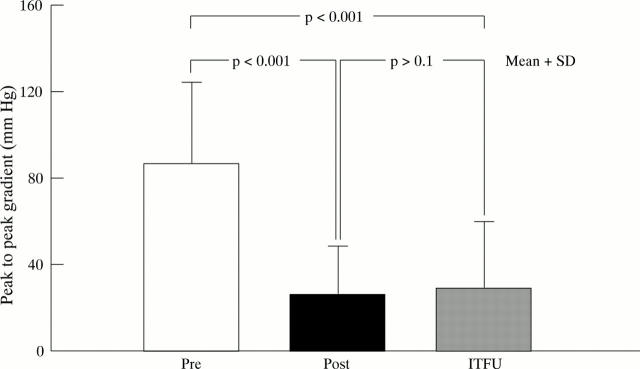
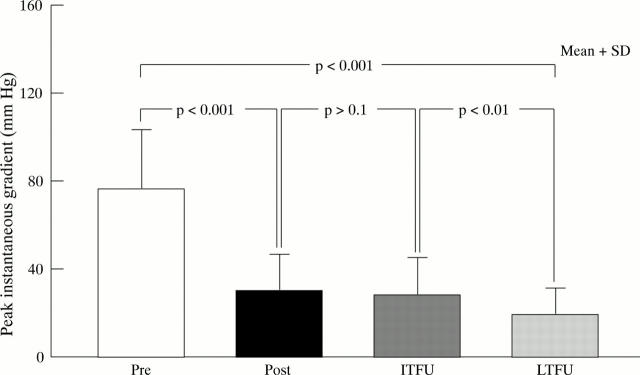
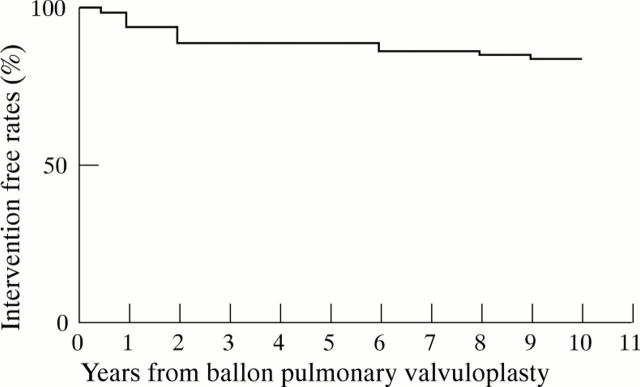
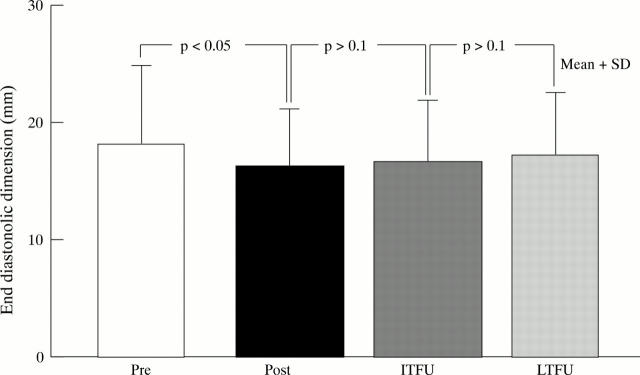
Methods and results: 85 patients (aged between 1 day and 20 years, mean (SD) 7.0 (6.4) years) underwent balloon dilatation of the pulmonary valve during an 11 year period ending August 1994. There was a resultant reduction in the peak to peak gradient from 87 (38) to 26 (22) mm Hg. Immediate surgical intervention was not required. Residual gradients of 29 (17) mm Hg were measured by catheterisation (n = 47) and echo Doppler (n = 82) at intermediate term follow up (two years). When individual results were scrutinised, nine of 82 patients had restenosis, defined as a peak gradient of 50 mm Hg or more. Seven of these patients underwent repeat balloon dilatation of the pulmonary valve: peak gradients were reduced from 89 (40) to 38 (20) mm Hg. Clinical evaluation and echo Doppler data of 80 patients showed that residual peak instantaneous Doppler gradients were 17 (15) mm Hg at long term follow up (three to 10 years, median seven), with evidence for late restenosis in one patient (1.3%). Surgical intervention was necessary to relieve fixed infundibular stenosis in three patients and supravalvar pulmonary stenosis in one. Repeat balloon dilatation was performed to relieve restenosis in two patients. Actuarial reintervention free rates at one, two, five, and 10 years were 94%, 89%, 88%, and 84%, respectively. Pulmonary valve regurgitation was noted in 70 of 80 patients at late follow up, but neither right ventricular dilatation nor paradoxical interventricular septal motion developed.
Conclusions: The results of late follow up of balloon dilatation of the pulmonary valve are excellent. Repeat balloon dilatation was performed in 11% of patients and surgical intervention for subvalvlar or supravalvar stenosis in 5%. Most patients had mild residual pulmonary regurgitation but right ventricular volume overload was not required. Balloon dilatation is the treatment of choice in the management of moderate to severe stenosis of the pulmonary valve. Further follow up studies should be undertaken to evaluate the significance of residual pulmonary regurgitation.
Figures
Similar articles
-
Balloon dilatation of the aortic valve after previous surgical valvotomy: immediate and follow up results.Br Heart J. 1994 Jun;71(6):558-60. doi: 10.1136/hrt.71.6.558. Br Heart J. 1994. PMID: 8043338 Free PMC article.
-
Follow-up results of balloon aortic valvuloplasty in children with special reference to causes of late aortic insufficiency.Am Heart J. 1997 Apr;133(4):418-27. doi: 10.1016/s0002-8703(97)70183-2. Am Heart J. 1997. PMID: 9124163
-
Long-term results (up to 17 years) of pulmonary balloon valvuloplasty in adults and its effects on concomitant severe infundibular stenosis and tricuspid regurgitation.Am Heart J. 2007 Mar;153(3):433-8. doi: 10.1016/j.ahj.2006.11.021. Am Heart J. 2007. PMID: 17307424
-
Percutaneous balloon pulmonary valvuloplasty: state of the art.Catheter Cardiovasc Interv. 2007 Apr 1;69(5):747-63. doi: 10.1002/ccd.20982. Catheter Cardiovasc Interv. 2007. PMID: 17330270 Review.
-
Long-term follow-up results after balloon dilatation of pulmonic stenosis, aortic stenosis, and coarctation of the aorta: a review.Prog Cardiovasc Dis. 1999 Jul-Aug;42(1):59-74. doi: 10.1016/s0033-0620(99)70009-5. Prog Cardiovasc Dis. 1999. PMID: 10505493 Review.
Cited by
-
Balloon Dilatation in the Management of Congenital Obstructive Lesions of the Heart: Review of Author's Experiences and Observations-Part II.J Cardiovasc Dev Dis. 2023 Jul 6;10(7):288. doi: 10.3390/jcdd10070288. J Cardiovasc Dev Dis. 2023. PMID: 37504544 Free PMC article. Review.
-
Balloon pulmonary valvuloplasty: A systematic review.Indian Heart J. 2024 Mar-Apr;76(2):86-93. doi: 10.1016/j.ihj.2023.12.007. Epub 2023 Dec 24. Indian Heart J. 2024. PMID: 38147974 Free PMC article.
-
Quadricuspid pulmonary valve stenosis treated by transcatheter pulmonary valvuloplasty with inoue balloon catheter.J Cardiol Cases. 2018 Aug 30;18(6):204-206. doi: 10.1016/j.jccase.2018.08.001. eCollection 2018 Dec. J Cardiol Cases. 2018. PMID: 30595773 Free PMC article.
-
Cardiopulmonary Function Assessment in Children With Pulmonary Valve Stenosis.Front Pediatr. 2022 Jan 14;9:802645. doi: 10.3389/fped.2021.802645. eCollection 2021. Front Pediatr. 2022. PMID: 35096713 Free PMC article.
-
Percutaneous balloon valvuloplasty with Inoue balloon catheter technique for pulmonary valve stenosis in adolescents and adults.Indian Heart J. 2017 Mar-Apr;69(2):176-181. doi: 10.1016/j.ihj.2016.11.316. Epub 2017 Mar 1. Indian Heart J. 2017. PMID: 28460765 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources