

Coronary artery stenting in unstable angina pectoris: a comparison with stable angina pectoris
- PMID: 10092566
- PMCID: PMC1729012
- DOI: 10.1136/hrt.81.4.393
Coronary artery stenting in unstable angina pectoris: a comparison with stable angina pectoris
Abstract
Objective: To compare early complication rates in unselected cases of coronary artery stenting in patients with stable v unstable angina.
Setting: Tertiary referral centre.
Patients: 390 patients with stable angina pectoris (SAP) and 306 with unstable angina (UAP). Patients treated for acute myocardial infarction (primary angioplasty) or cardiogenic shock were excluded.
Interventions: 268 coronary stents were attempted in 211 patients (30.3%). Stents used included AVE (63%), Freedom (14%), NIR (7%), Palmaz-Schatz (5%), JO (5%), and Multilink (4%). Intravascular ultrasound was not used in any of the cases. All stented patients were treated with ticlopidine and aspirin together with periprocedural unfractionated heparin.
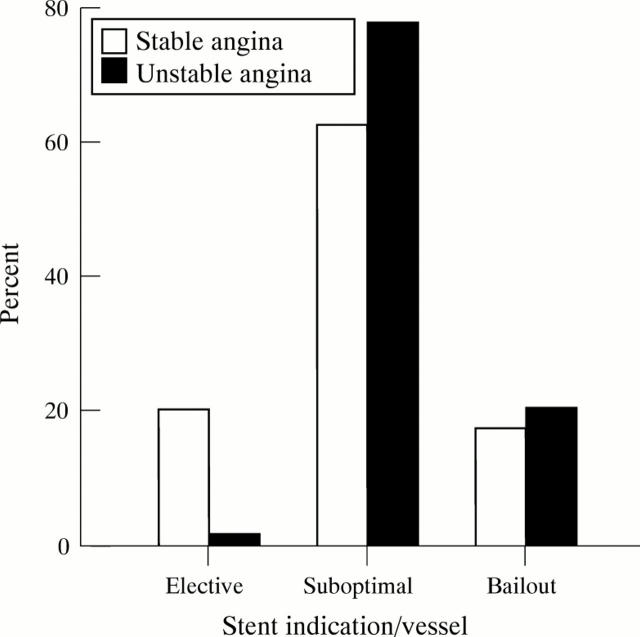
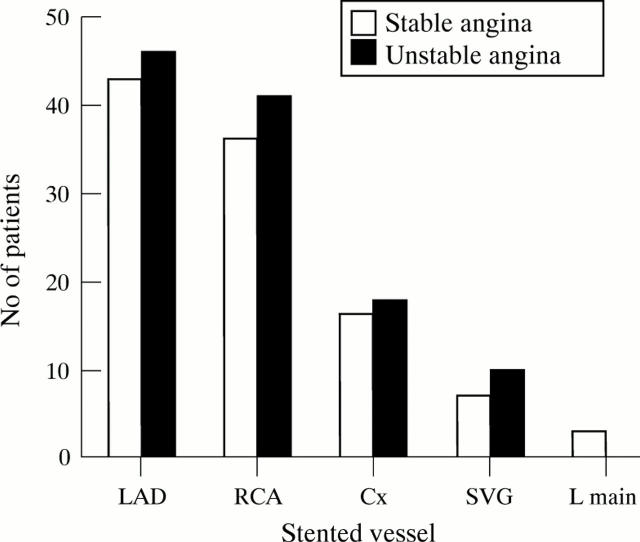
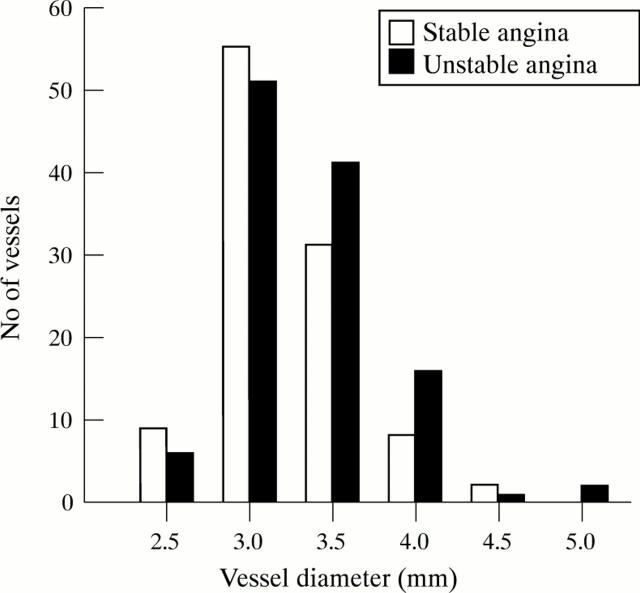
Results: 123 stents were successfully deployed in 99 SAP patients v 132 stents in 103 UAP patients. Failed deployment occurred with nine stents in SAP patients, v four in UAP patients (NS). Stent thrombosis occurred in four SAP patients and 11 UAP patients. Multivariate analysis showed no relation between stent thrombosis and clinical presentation (SAP v UAP), age, sex, target vessel, stent length, or make of stent. Stent thrombosis was associated with small vessel size (p < 0.001) and bailout stenting (p = 0.01) compared with elective stenting and stenting for suboptimal PTCA, with strong trends toward smaller stent diameter (p = 0.052) and number of stents deployed (p = 0.06). Most stent thromboses occurred in vessels < 3 mm diameter.
Conclusions: Coronary artery stenting in unstable angina is safe in vessels >/= 3 mm diameter, with comparable initial success and stent thrombosis rates to stenting in stable angina.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous