

Review
doi: 10.1111/j.1469-7793.1999.0631u.x.
Molecular insights into the physiology of the 'thin film' of airway surface liquid
Affiliations
- PMID: 10200413
- PMCID: PMC2269304
- DOI: 10.1111/j.1469-7793.1999.0631u.x
Item in Clipboard
Review
Molecular insights into the physiology of the 'thin film' of airway surface liquid
J Physiol.
.
Abstract
The epithelia that line the airways of the lung exhibit two general functions: (1) airway epithelia in all regions 'defend' the lung against infectious and noxious agents; and (2) airway epithelia in the proximal regions replenish water lost from airway surfaces, i.e. the 'insensible water loss', consequent to conditioning inspired air. How airway epithelia perform both functions, and co-ordinate them in health and disease, is the subject of this review.
Figures
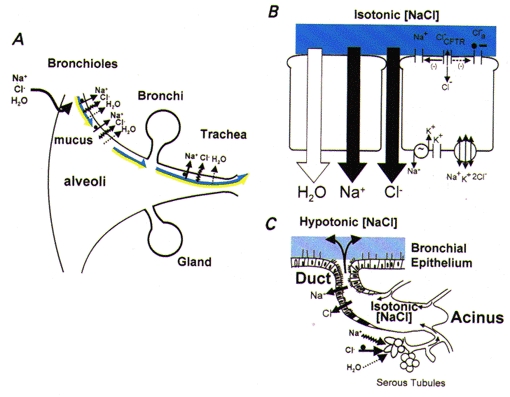
A, organ-level description. The relative surface areas (not to scale) of the different regions are shown. Both components of ASL are represented as being transported cephalad on pulmonary surfaces (bicoloured arrows: dark blue, isotonic PCL component; yellow, mucous component). In the airways, the mechanisms for absorption from ASL are driven by active Na+ absorption, with Cl− and water accompanying passively. The bronchioles are shown as absorptive. Liquid could be secreted in either very distal bronchiolar regions or, as depicted, on alveolar surfaces. B, model of superficial airway epithelial cells mediating isotonic volume transport. The basolateral Na+-K+-ATPase generates the driving force for Na+ entry across the apical membrane, which is mediated by ENaCs. Both functions of CFTR, as a Cl− channel () and as regulator of ENaC (Na+), and the alternative (Ca2+-activated) Cl− channel (Cl−a) are depicted on the apical membrane. Active Na+ absorption is transcellular, whereas anion flow is, in part, cellular and, in larger part, transcellular. The epithelium is quite permeable to water, permitting isosmotic volume transport. Hence, the ASL is designated as isotonic [NaCl] (depicted in dark blue). C, submucosal gland. Isotonic volume secretion in the acinus is illustrated mediated by active Cl− secretion coupled with passive Na+ and water secretion, which probably reflects a significant contribution from serous tubules expressing CFTR located in the acinar region. The gland ducts are represented as absorbing NaCl, but not water, resulting in a hypotonic secretion (depicted in light blue).
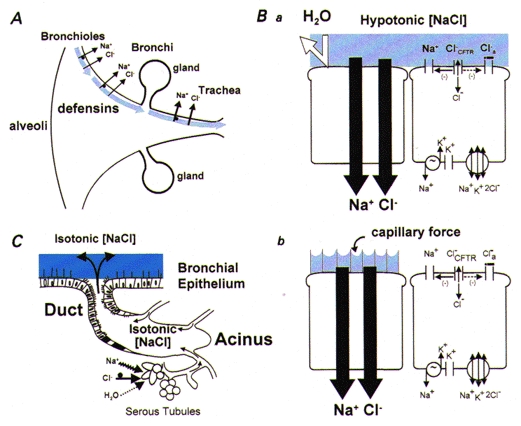
A, organ-level description. The epithelium lining airway surfaces is represented as absorbing NaCl but not water from ASL (shown as light blue to indicate hypotonicity). Antimicrobial substances (defensins) are shown, which are active in this ‘low salt’ environment. No arrows depicting surface liquid clearance are shown, due to the inability of the cell models (see below) to deal with volume absorption or a mucous layer. B, cell models postulated to explain the production of hypotonic ASL. Ba, the ‘sweat ductal model’. The key elements are the transcellular absorption of Na+ (via ENaC) and Cl− (via CFTR) and epithelial water impermeability (depicted as ‘deflected’ arrow). Bb, the ‘surface forces’ model. Outstretched cilia are depicted on the left cell that generate small radius (< 0.1 μm) menisci at an air-water interface of high surface tension. NaCl is absorbed transcellularly and the osmotic force generated to absorb H2O from the airway surface is balanced by ‘capillary’ forces generated by the menisci, resulting in a low [NaCl] ASL. C, submucosal glands. Based on previous reports (Quinton, 1979), this model might predict isotonic gland secretion. Presumably, this process adds volume to the surface and compositional modification (lowering [NaCl]) is performed by the superficial epithelium.
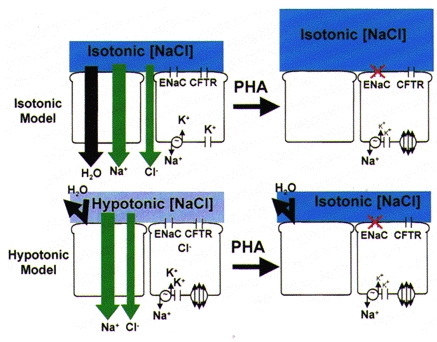
Upper panel, the isotonic model predicts that loss of transepithelial Na+ absorption will abolish most volume absorption and increase the volume of isotonic liquid (shown in dark blue) on epithelial surfaces. Lower panel, the hypotonic model predicts that NaCl absorption but not volume (H2O) absorption will be perturbed in PHA, resulting in conversion of ASL from hypotonic (‘low salt’, shown in light blue) to isotonic (‘high salt’, shown in dark blue) ASL with no change in volume.
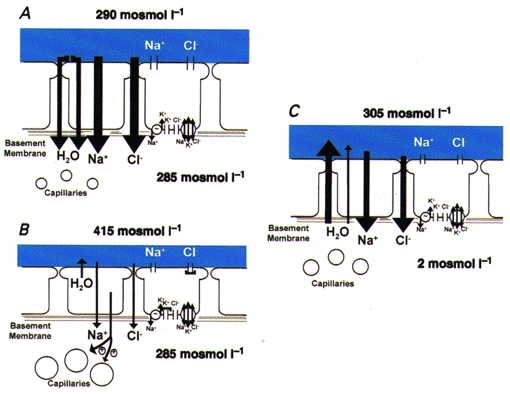
A, airway epithelium under basal conditions (osmolarity of the ASL slightly exceeds that of the interstitium). B, consequent to accelerated evaporative water loss, the volume of ASL is reduced and NaCl becomes concentrated, which provides the osmotic driving force (depicted as osmolarity raised to 415 mosmol l−1) that leads to (1) epithelial shrinkage, (2) slowing of active ion absorption (depicted as smaller vectors) consequent to inhibition of apical Cl− channels and basolateral K+ channels (depicted as ‘caps’ on channel pores), and (3) signalling, via a nitric oxide synthase-mediated system to the submucosal microvasculature to promote dilatation. C, restoration of water to airway surface. Water moves from the interstitium across the epithelium via cellular and perhaps paracellular routes in response to the luminal solution osmolar gradient to replenish the volume of ASL.
References
-
- Anderson MP, Gregory RJ, Thompson S, Souza DW, Paul S, Mulligan RC, Smith AE, Welsh MJ. Demonstration that CFTR is a chloride channel by alteration of its anion selectivity. Science. 1991;253:202–205. - PubMed
-
- Bear CE, Li C, Kartner N, Bridges RJ, Jensen TJ, Ramjeesingh M, Riordan JR. Purification and functional reconstitution of the cystic fibrosis transmembrane conductance regulator (CFTR) Cell. 1992;68:809–818. - PubMed
-
- Boucher RC. Human airway ion transport (Part 1) American Journal of Respiratory and Critical Care Medicine. 1994;150:271–281. - PubMed
-
- Boucher RC, Stutts MJ, Bromberg PA, Gatzy JT. Regional differences in airway surface liquid composition. Journal of Applied Physiology. 1981;50:613–620. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources