

The relation between purulent manifestations and antibiotic treatment of upper respiratory tract infections
- PMID: 10203620
- PMCID: PMC1496549
- DOI: 10.1046/j.1525-1497.1999.00306.x
The relation between purulent manifestations and antibiotic treatment of upper respiratory tract infections
Abstract
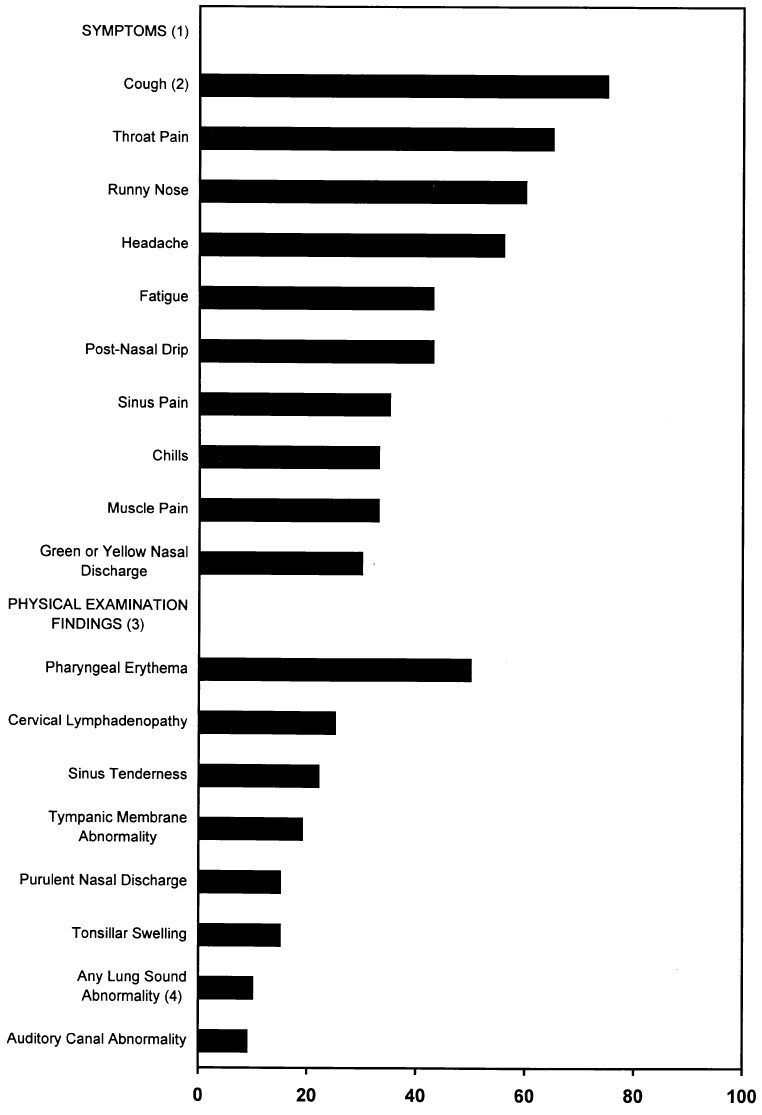
Objective: To describe the clinical features of patients diagnosed with upper respiratory tract infections (URIs), and determine which clinical features are associated with antibiotic use.
Design: Prospective cohort study.
Setting: Three ambulatory care practices at a group-model HMO in the Denver metropolitan area.
Patients: Adults (aged 18 years or older) seeking care for acute respiratory illnesses.
Measurements: Clinical features were documented on standardized encounter forms. Clinician type, secondary diagnoses, and antibiotic treatment were extracted from administrative databases. Results are presented as adjusted odds ratios (ORs) with 95% confidence intervals (CIs).
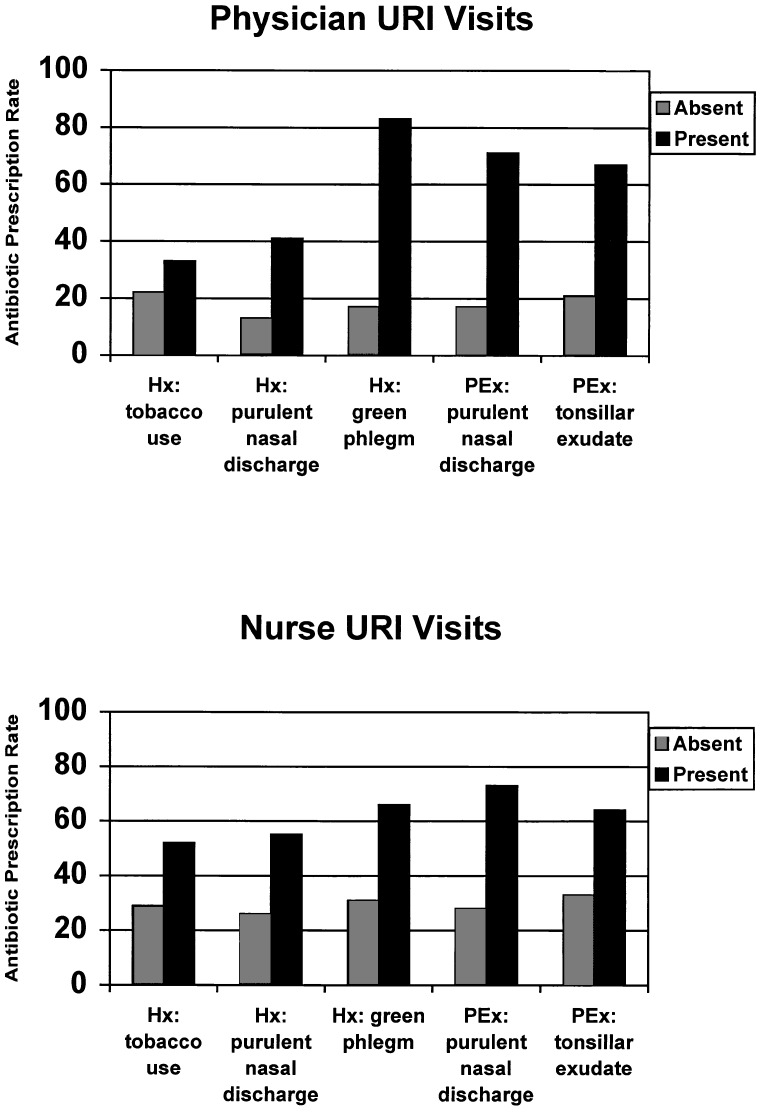
Main results: Antibiotics were prescribed to 33% (95% CI 28%, 38%) of patients diagnosed with URI, after excluding patients with coexisting antibiotic-responsive conditions (e.g., sinusitis, pharyngitis) or a history of cardiopulmonary disease. Multivariate logistic regression analysis identified tobacco use (OR 2.8; 95% CI 1.5, 5.1), history of purulent nasal discharge (OR 2.0; 95% CI 1.1, 3.6) or green phlegm (OR 4.8; 95% CI 2.1, 11.1), and examination findings of purulent nasal discharge (OR 5.2; 95% CI 2.4, 11.2) or tonsillar exudate (OR 3.7; 95% CI 1.1, 12.1) to be independently associated with antibiotic use. The majority of patients treated with antibiotics (82%) had at least one of these factors present.
Conclusions: Antibiotic treatment of URIs is most common when purulent manifestations are present. Efforts to reduce antibiotic treatment of URIs should educate clinicians about the limited value of purulent manifestations in predicting antibiotic-responsive disease.
Figures
Comment in
-
Managing upper respiratory tract infections: practice without evidence.J Gen Intern Med. 1999 Mar;14(3):203-4. doi: 10.1046/j.1525-1497.1999.00315.x. J Gen Intern Med. 1999. PMID: 10203630 Free PMC article. No abstract available.
References
-
- Evans AS. Clinical syndromes in adults caused by respiratory infection. Med Clin North Am. 1967;51:803–29. - PubMed
-
- Schappert SM. Ambulatory care visits to physician offices, hospital outpatient departments, and emergency departments: United States, 1995. National Center for Health Statistics. Vital Health Stat 13. 1997:129. - PubMed
-
- Gonzales R, Steiner JF, Sande MA. Antibiotic prescribing for adults with colds, upper respiratory infections and bronchitis by ambulatory physicians in the United States. JAMA. 1997;278:901–4. - PubMed
-
- Mainous AG, III, Hueston WJ, Clark JR. Antibiotics and upper respiratory infection: do some folks think there is a cure for the common cold? J Fam Pract. 1996;42:357–61. - PubMed
-
- McCaig LF, Hughes JM. Trends in antimicrobial drug prescribing among office-based physicians in the United States. JAMA. 1995;273:214–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical