

Double blind, randomised study of continuous terbinafine compared with intermittent itraconazole in treatment of toenail onychomycosis. The LION Study Group
- PMID: 10205099
- PMCID: PMC27831
- DOI: 10.1136/bmj.318.7190.1031
Double blind, randomised study of continuous terbinafine compared with intermittent itraconazole in treatment of toenail onychomycosis. The LION Study Group
Abstract
Objective: To compare the efficacy and safety of continuous terbinafine with intermittent itraconazole in the treatment of toenail onychomycosis.
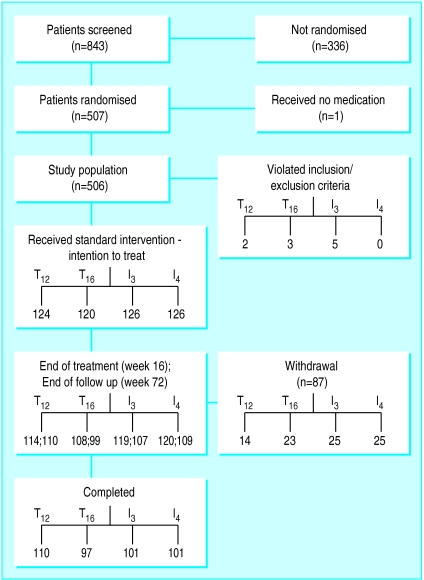
Design: Prospective, randomised, double blind, double dummy, multicentre, parallel group study lasting 72 weeks.
Setting: 35 centres in six European countries.
Subjects: 496 patients aged 18 to 75 years with a clinical and mycological diagnosis of dermatophyte onychomycosis of the toenail.
Interventions: Study patients were randomly divided into four parallel groups to receive either terbinafine 250 mg a day for 12 or 16 weeks (groups T12 and T16) or itraconazole 400 mg a day for 1 week in every 4 weeks for 12 or 16 weeks (groups I3 and I4).
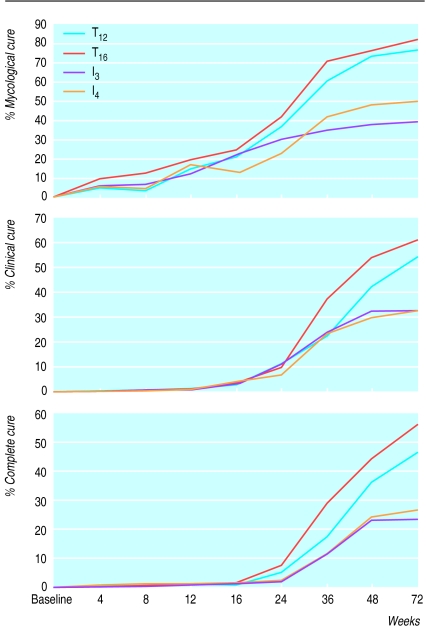
Main outcome measures: Assessment of primary efficacy at week 72 was mycological cure, defined as negative results on microscopy and culture of samples from the target toenail.
Results: At week 72 the mycological cure rates were 75.7% (81/107) in the T12 group and 80. 8% (80/99) in the T16 group compared with 38.3% (41/107) in the I3 group and 49.1 % (53/108) in the I4 group. All comparisons (T12 v I3, T12 v I4, T16 v I3, T16 v I4) showed significantly higher cure rates in the terbinafine groups (all P<0.0001). Also, all secondary clinical outcome measures were significantly in favour of terbinafine at week 72. There were no differences in the number or type of adverse events recorded in the terbinafine or itraconazole groups.
Conclusion: Continuous terbinafine is significantly more effective than intermittent itraconazole in the treatment of patients with toenail onychomycosis.
Figures
Comment in
-
Treatment of toenail onychomycosis. Will Paper's key message soon appear in promotional material for drug?BMJ. 1999 Oct 30;319(7218):1196-7. doi: 10.1136/bmj.319.7218.1196a. BMJ. 1999. PMID: 10541522 Free PMC article. No abstract available.
-
Treatment of toenail onychomycosis. Do crinkly toenails really matter?BMJ. 1999 Oct 30;319(7218):1197. BMJ. 1999. PMID: 10610151 No abstract available.
-
Treatment of toenail onychomycosis. Prescribing terbinafine to every patient with the condition would be expensive.BMJ. 1999 Oct 30;319(7218):1197. BMJ. 1999. PMID: 10610152 No abstract available.
-
Treatment of toenail onychomycosis. Roughly quarter of BMJ staff surveyed said they had crinkly toenails.BMJ. 1999 Oct 30;319(7218):1197. BMJ. 1999. PMID: 10610153 No abstract available.
-
Crinkly toenails. Toenail onychomycosis can cause serious problems.BMJ. 2000 Feb 12;320(7232):448. BMJ. 2000. PMID: 10669462 Free PMC article. No abstract available.
References
-
- Roberts DT. Prevalence of dermatophyte onychomycosis in the United Kingdom: results of an omnibus survey. Br J Dermatol. 1992;126(suppl 39):23–27. - PubMed
-
- Sais G, Jugglà A, Peyrí J. Prevalence of dermatophyte onychomycosis in Spain: a cross-sectional study. Br J Dermatol. 1995;132:758–761. - PubMed
-
- Editorial. Prevalence, morbidity and cost of dermatological diseases. J Invest Dermatol. 1979;73:395–401. - PubMed
-
- Heikkilä H, Stubb S. The prevalence of onychomycosis in Finland. Br J Dermatol. 1995;133:699–703. - PubMed
-
- de Backer M, de Keyser P, de Vroey C, Lesaffre E. A 12-week treatment for dermatophyte toe onychomycosis: terbinafine 250 mg/day vs itraconazole 200 mg/day—a double blind comparative trial. Br J Dermatol. 1996;134(suppl 136):16–17. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources