

Reducing the risk of major elective surgery: randomised controlled trial of preoperative optimisation of oxygen delivery
- PMID: 10213716
- PMCID: PMC27840
- DOI: 10.1136/bmj.318.7191.1099
Reducing the risk of major elective surgery: randomised controlled trial of preoperative optimisation of oxygen delivery
Abstract
Objectives: To determine whether preoperative optimisation of oxygen delivery improves outcome after major elective surgery, and to determine whether the inotropes, adrenaline and dopexamine, used to enhance oxygen delivery influence outcome.
Design: Randomised controlled trial with double blinding between inotrope groups.
Setting: York District Hospital, England.
Subjects: 138 patients undergoing major elective surgery who were at risk of developing postoperative complications either because of the surgery or the presence of coexistent medical conditions.
Interventions: Patients were randomised into three groups. Two groups received invasive haemodynamic monitoring, fluid, and either adrenaline or dopexamine to increase oxygen delivery. Inotropic support was continued during surgery and for at least 12 hours afterwards. The third group (control) received routine perioperative care.
Main outcome measures: Hospital mortality and morbidity.
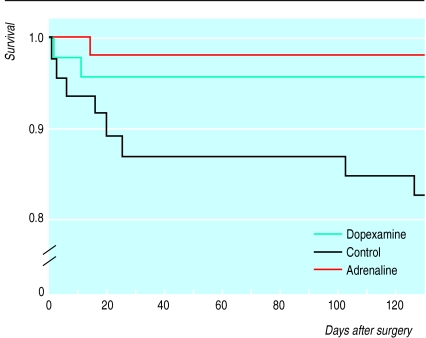
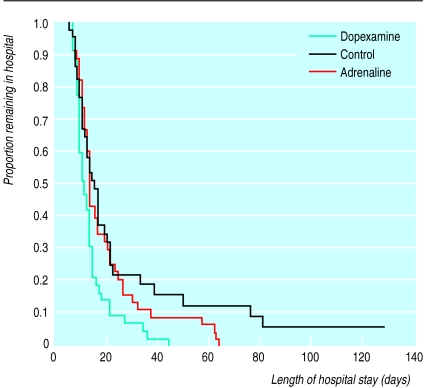
Results: Overall, 3/92 (3%) preoptimised patients died compared with 8/46 controls (17%) (P=0.007). There were no differences in mortality between the treatment groups, but 14/46 (30%) patients in the dopexamine group developed complications compared with 24/46 (52%) patients in the adrenaline group (difference 22%, 95% confidence interval 2% to 41%) and 28 patients (61%) in the control group (31%, 11% to 50%). The use of dopexamine was associated with a decreased length of stay in hospital.
Conclusion: Routine preoperative optimisation of patients undergoing major elective surgery would be a significant and cost effective improvement in perioperative care.
Figures
Comment in
-
Reducing the risk of major elective surgery.BMJ. 1999 Apr 24;318(7191):1087-8. doi: 10.1136/bmj.318.7191.1087. BMJ. 1999. PMID: 10213694 Free PMC article. No abstract available.
-
Reducing the risk of major elective surgery. Paper should have given details on causes of death.BMJ. 1999 Nov 20;319(7221):1369; author reply 1370-1. doi: 10.1136/bmj.319.7221.1369a. BMJ. 1999. PMID: 10567159 Free PMC article. No abstract available.
-
Reducing the risk of major elective surgery. These results must now be put into clinical practice.BMJ. 1999 Nov 20;319(7221):1370; author reply 1370-1. BMJ. 1999. PMID: 10617343 No abstract available.
-
Reducing the risk of major elective surgery. What exactly reduces the risk?BMJ. 1999 Nov 20;319(7221):1370-1. BMJ. 1999. PMID: 10617344 No abstract available.
-
Reducing the risk of major elective surgery. Better management of intensive care unit beds is necessary.BMJ. 1999 Nov 20;319(7221):1369-70; disscussion 1370-1. BMJ. 1999. PMID: 11123879 No abstract available.
References
-
- Campling EA, Devlin HB, Hoile RW, Lunn JN. London: Royal College of Surgeons; 1992. National Confidential Enquiry into Perioperative Deaths. - PubMed
-
- Shoemaker WC, Appel PL, Kram HB, Waxman K, Lee T. Prospective trial of supranormal values of survivors as therapeutic goals in high-risk surgical patients. Chest. 1987;94:1176–1186. - PubMed
-
- Boyd O, Grounds RM, Bennett ED. A randomised clinical trial of the effect of deliberate perioperative increase of oxygen delivery on mortality in high-risk surgical patients. JAMA. 1993;270:2699–2707. - PubMed
-
- Mythen MG, Webb AR. The role of gut mucosal hypoperfusion in the pathogenesis of post-operative organ dysfunction. Intensive Care Med. 1994;20:203–209. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical