

Factors influencing successful angiographic occlusion of aneurysms treated by coil embolization
- PMID: 10219403
- PMCID: PMC7056068
Factors influencing successful angiographic occlusion of aneurysms treated by coil embolization
Abstract
Background and purpose: Coil embolization of berry aneurysms is a relatively new treatment whose long-term efficacy has yet to be established. The purpose of this study was, first, to attempt to identify factors that might be important in predicting success both at the time of treatment and at the time of follow-up angiography, and, second, to study changes in the aneurysm between treatment and follow-up to determine the frequency of these changes.
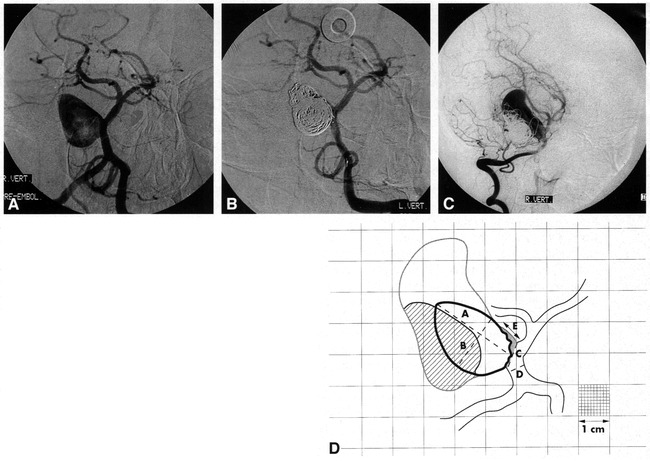
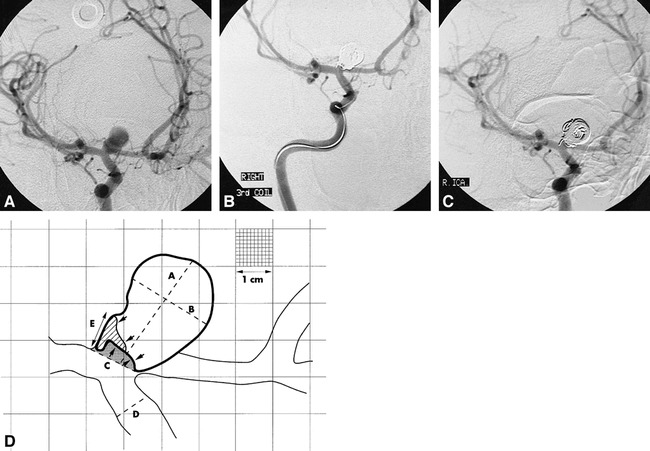
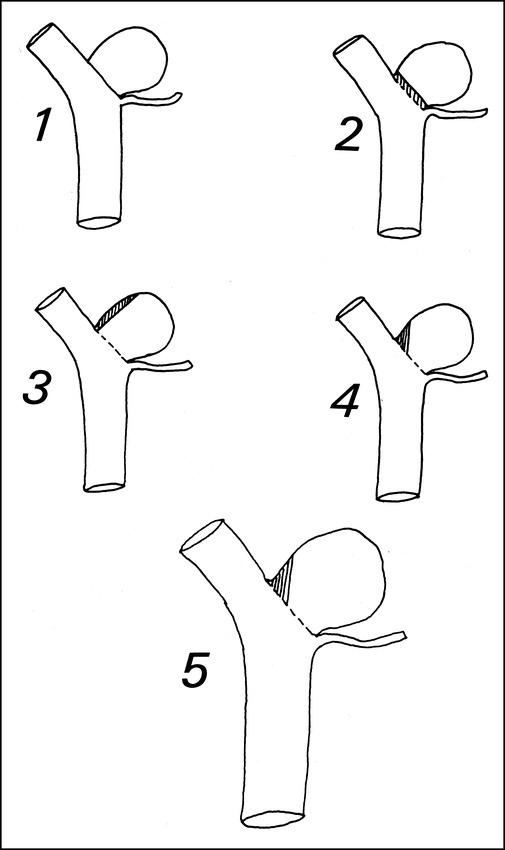
Methods: The pretreatment, posttreatment, and follow-up angiograms of the first 63 aneurysms (in 58 patients) treated at our institution between June 1992 and April 1995 were analyzed, and the percentage of occlusion of each aneurysm was calculated. The size of any rest was noted for the posttreatment and follow-up angiograms. Treatment success was defined as a residue of less than 2 mm. Aneurysms were said to have changed if the percentage of occlusion had altered by more than 2.5% or if the difference in rest size was greater than 0.25 mm. Possible factors influencing primary and follow-up success rates were correlated against these calculations.
Results: Success rates at treatment and follow-up were 71% and 65%, respectively. No change occurred in 41% of aneurysms, and 20% had a decrease in size of the residue. Twenty-eight percent had coil compaction, and 11% had aneurysmal growth. Neck size was the only significant variable in primary treatment success. Success at follow-up correlated significantly with neck size, initial treatment success, vasospasm at the time of treatment, and clinical presentation.
Conclusion: Best long-term angiographic results are obtained when the primary treatment is successful, when the aneurysm is small and narrow-necked, when the acutely ruptured aneurysm is treated within 15 days of ictus, and with anterior communicating and basilar-tip aneurysms.
Figures
References
-
- Byrne JV, Adams CBT, Kerr RSC, et al. Endovascular treatment of inoperable intracranial aneurysms with platinum coils. Br J Neurosurg 1995;9:585-592 - PubMed
-
- Casasco AE, Aymard A, Gobin YP, et al. Selective endovascular treatment of 71 intracranial aneurysms with platinum coils. J Neurosurg 1993;79:3-10 - PubMed
-
- Guglielmi G, Vinuela F, Dion J, Duckwiler G. Electrothrombosis of saccular aneurysms via endovascular approach, part 2: preliminary clinical experience. J Neurosurg 1991;75:8-14 - PubMed
-
- Guglielmi G, Vinuela F, Duckwiler G, et al. Endovascular treatment of posterior circulation aneurysms by electrothrombosis using electrically detachable coil. J Neurosurg 1992;77:515-524 - PubMed
-
- Chyatte D. The epidemiology, genetics, and clinical behavior of intracranial aneurysms. In: Awad IA, ed. Current Management of Cerebral Aneurysms. Neurosurgical Topics Series, bk 15. Park Ridge, IL: American Association of Neurological Surgeons; 1993;1-20
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous