

Distinct immunoglobulin class and immunoglobulin G subclass patterns against ganglioside GQ1b in Miller Fisher syndrome following different types of infection
- PMID: 10225903
- PMCID: PMC115986
- DOI: 10.1128/IAI.67.5.2414-2420.1999
Distinct immunoglobulin class and immunoglobulin G subclass patterns against ganglioside GQ1b in Miller Fisher syndrome following different types of infection
Abstract
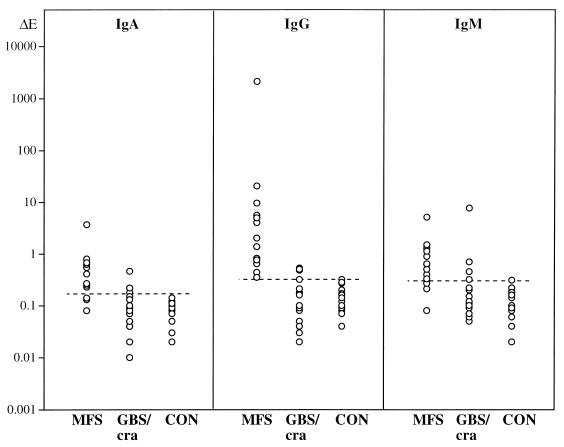
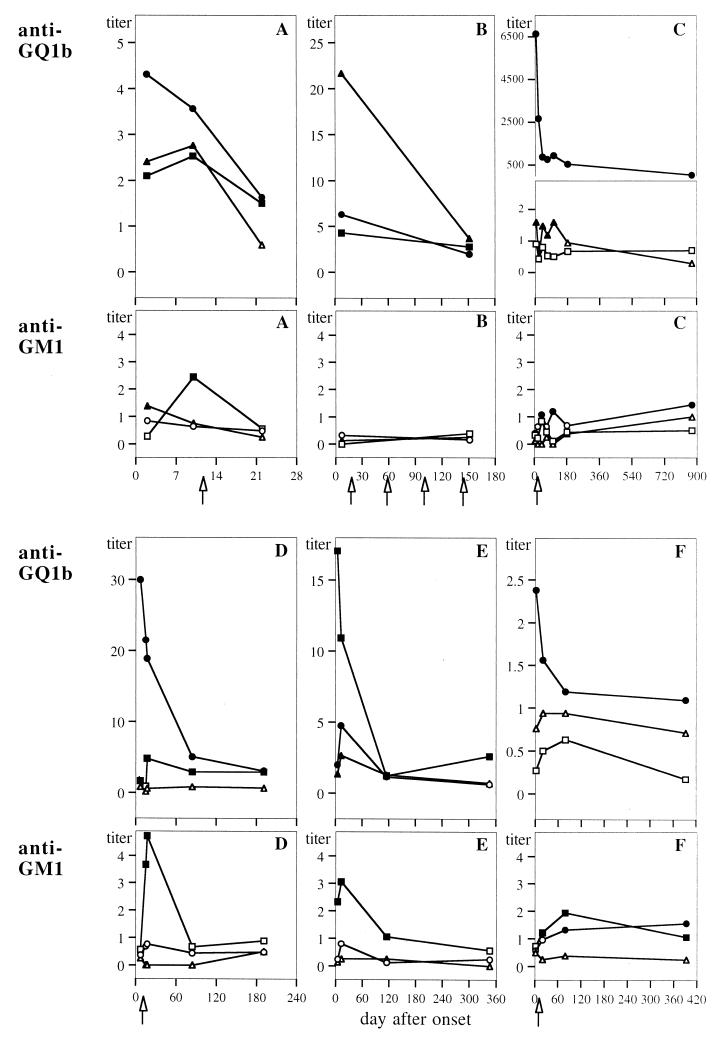
We studied serum antibodies against gangliosides GQ1b and GM1 in 13 patients with Miller Fisher syndrome (MFS) and in 18 patients with Guillain-Barré syndrome (GBS) with cranial nerve involvement. Anti-GQ1b titers were elevated in all patients with MFS cases (immunoglobulin G [IgG] > IgA, IgM), and in 8 of the 18 with GBS. Lower frequencies of increased anti-GM1 titers were observed in MFS patients (3 of 13), as well as in GBS patients (5 of 18). During the course of MFS, anti-GQ1b titers of all Ig classes decreased within 3 weeks after onset. By contrast, anti-GM1 titers (mainly IgM) transiently increased during the course of MFS in five of six patients, suggesting a nonspecific secondary immune response. In patients with MFS following respiratory infections, IgG was the major anti-GQ1b Ig class (six of six patients) and IgG3 was the major subclass (five of six). In contrast, four of five patients with MFS following gastrointestinal infections showed predominance of anti-GQ1b IgA or IgM over IgG and predominance of the IgG2 subclass; anti-GQ1b IgG (IgG3) prevailed in one patient only. These distinct Ig patterns strongly suggest that different infections may trigger different mechanisms of anti-GQ1b production, such as via T-cell-dependent as opposed to T-cell-independent pathways. Thus, the origin of antibodies against GQ1b in MFS may be determined by the type of infectious agent that precipitates the disease.
Figures
References
-
- Asbury A K, Cornblath D R. Assessment of current diagnostic criteria for Guillain-Barré syndrome. Ann Neurol. 1990;27(Suppl.):S21–S24. - PubMed
-
- Aspinall G O, McDonald A G, Pang H, Kurjanczyk L A, Penner J L. Lipopolysaccharides of Campylobacter jejuni serotype O:19: structures of core oligosaccharide regions from the serostrain and two bacterial isolates from patients with the Guillain-Barré syndrome. Biochemistry. 1994;33:241–249. - PubMed
-
- Bech E, Orntoft T F, Andersen L P, Skinhoj P, Jakobsen J. IgM anti-GM1 antibodies in the Guillain-Barré syndrome: a serological predictor of the clinical course. J Neuroimmunol. 1997;72:59–66. - PubMed
-
- Berlit P, Rakicky J. The Miller Fisher syndrome: review of the literature. J Clin Neuro-Ophthalmol. 1992;12:57–63. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
