

Pain-mediated altered absorption and metabolism of ibuprofen: an explanation for decreased serum enantiomer concentration after dental surgery
- PMID: 10233203
- PMCID: PMC2014238
- DOI: 10.1046/j.1365-2125.1999.00902.x
Pain-mediated altered absorption and metabolism of ibuprofen: an explanation for decreased serum enantiomer concentration after dental surgery
Abstract
Aims: Rapid onset of analgesia is essential in the treatment of acute pain. There is evidence that conditions of stress cause delayed and decreased pain relief from oral analgesic products through impaired absorption. The aim was to determine the effect of surgery for removal of wisdom teeth on the plasma concentration-time profile of ibuprofen enantiomers.
Methods: Racemic ibuprofen, 200 mg in one group (n=7) and 600 mg in another group (n=7) was administered 1 week before (control) and again after (test) surgical removal of wisdom teeth. Serum concentrations of ibuprofen enantiomers were measured for 6 h.
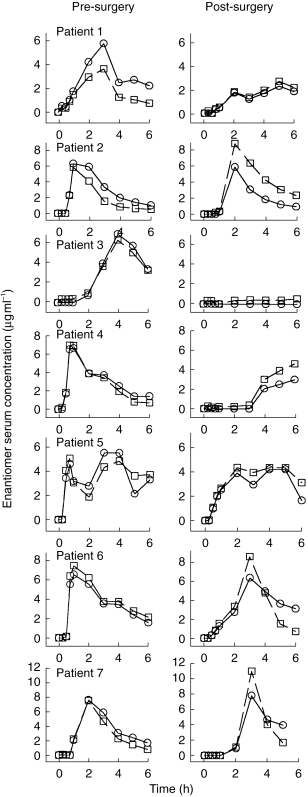
Results: During the control phase, S- and R-ibuprofen concentrations were within the suggested therapeutic range. Surgery resulted in a 2 h delay in the mean time to peak concentration, significant decreases in serum ibuprofen concentration following both doses, and a fall to sub-optimal serum concentrations following the 200 mg dose. During the first 2 h after the 200 mg dose, dental extraction resulted in a significant reduction of the area under serum drug concentration (AUC (0, 2 h) mg l-1 h) from 5.6+/-2.9 to 1.6+/-1.8 (P<0.01) and from 5.5+/-3.0 to 2.1+/-2.0 (P<0.05) for S and R-ibuprofen, respectively. Similar observations were made following the 600 mg dose for AUC (0, 2 h) of S-ibuprofen (from 14.2+/-6.1 to 7.2+/-5.5 mg l-1 h, P<0.05) with no significant difference for R-ibuprofen (from 14.4+/-9.5 to 5.8+/-7. 1). AUC (0, 6 h) was also significantly reduced by surgery. The pattern of stereoselectivity in serum ibuprofen concentration was reversed by surgery such that the S enantiomer was predominant in the control phase but not in the post-surgery phase, which is suggestive of reduced metabolic chiral inversion.
Conclusions: Surgery for wisdom tooth removal resulted in substantial decreases in the serum concentration of ibuprofen enantiomers and a prolongation in the time to peak concentration. Reduced absorption and altered metabolism are the likely cause of these changes. Thus, dental patients may experience a delayed response and possible treatment failure when taking ibuprofen for pain relief after surgery. Our observation may have implications for the treatment of other diseases.
Figures



References
-
- Laska EM, Sunshine A, Marrero I, Olson N, Siegel C, McCormick N. The correlation between blood levels of ibuprofen and clinical analgesic response. Clin Pharmacol Ther. 1986;40:1–7. - PubMed
-
- Seymour RA, Kelly PJ, Hawkesford JE. Pharmacokinetics and efficacy of low-dose ketoprofen in prospective dental pain. Clin Drug Invest. 1998;15:279–284. - PubMed
-
- Goldstein DJ, Brunelle RL, George RE, et al. Picenadol in large multicenter dental pain study. Pharmacotherapy. 1994;14:54–59. - PubMed
-
- Wright MR, Sattari S, Brocks DR, Jamali F. An improved assay for the enantiomers of ibuprofen. J Chromatogr. 1992;583:259–265. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
