

Pancreaticoduodenectomy with or without extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma: comparison of morbidity and mortality and short-term outcome
- PMID: 10235519
- PMCID: PMC1420805
- DOI: 10.1097/00000658-199905000-00003
Pancreaticoduodenectomy with or without extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma: comparison of morbidity and mortality and short-term outcome
Abstract
Objective: This prospective, randomized, single-institution trial was designed to evaluate the end points of mortality, morbidity, and survival in patients undergoing standard versus radical (extended) pancreaticoduodenectomy (including distal gastrectomy and retroperitoneal lymphadenectomy).
Summary background data: Numerous retrospective reports and one prospective randomized trial have suggested that the performance of an extended lymphadenectomy in association with a pancreaticoduodenal resection may improve long-term survival for some patients with pancreatic and other periampullary adenocarcinomas. Many of these previously published studies can be criticized for their retrospective and nonrandomized designs, for the inclusion of nonconcurrent control groups, and for their small numbers.
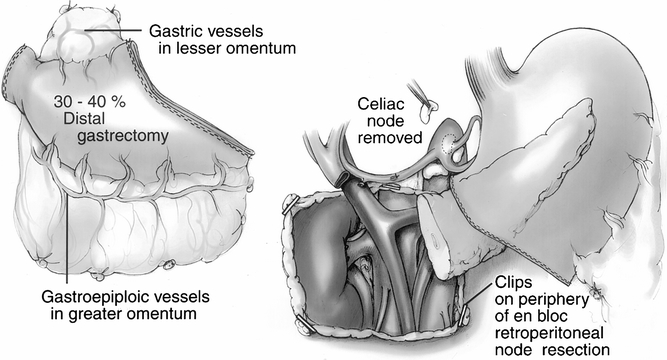
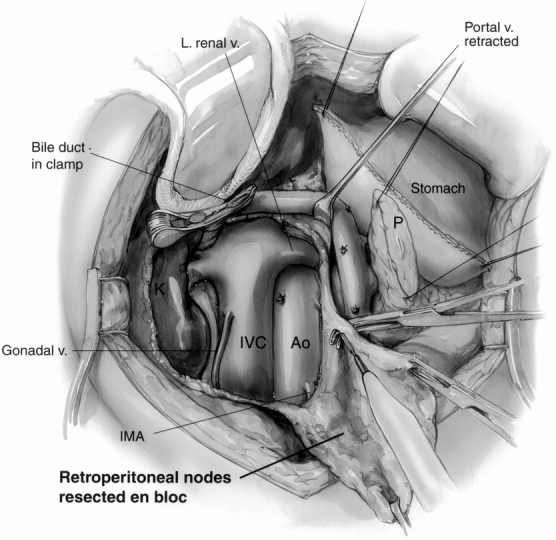
Methods: Between April 1996 and December 1997, 114 patients with periampullary adenocarcinoma were enrolled in an ongoing, prospective, randomized trial at The Johns Hopkins Hospital. After intraoperative verification of completely resected periampullary adenocarcinoma, the patients were randomized to receive either a standard pancreaticoduodenectomy (removing only the peripancreatic lymph nodes en bloc with the specimen) or a radical pancreaticoduodenectomy (standard resection plus distal gastrectomy and retroperitoneal lymphadenectomy). All pathology specimens were reviewed and categorized. The postoperative morbidity, mortality, and short-term outcomes were examined.
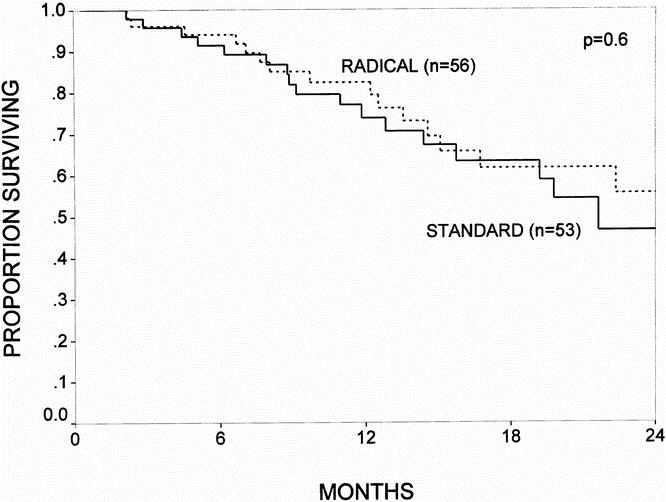
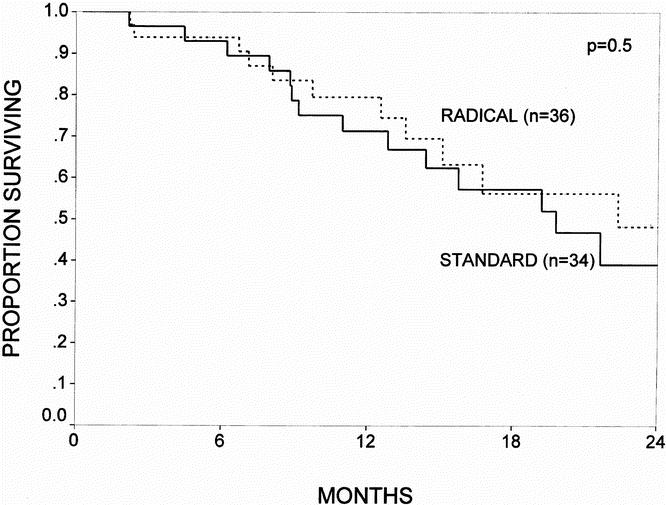
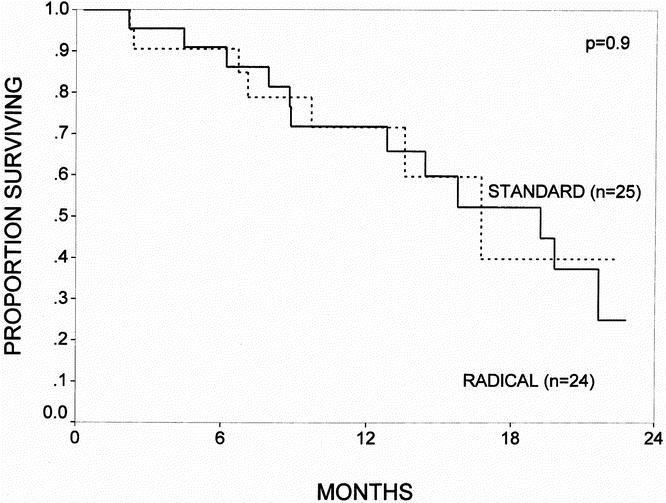
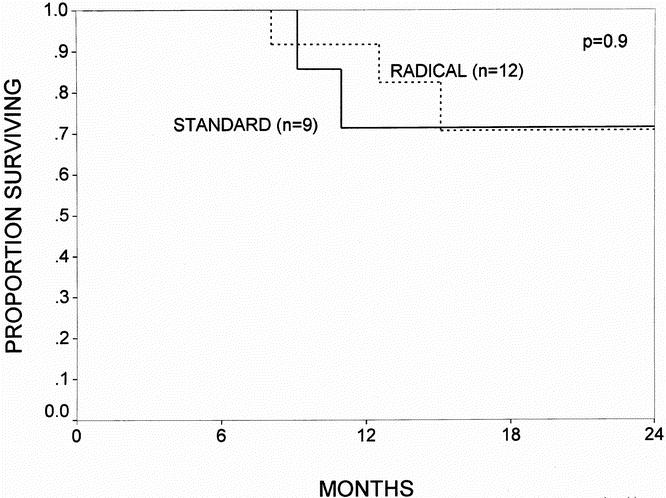
Results: Of the 114 patients randomized, 56 underwent a standard pancreaticoduodenectomy and 58 a radical pancreaticoduodenectomy. The two groups were statistically similar with regard to age and gender, but there was a higher percentage of white patients in the radical group. All the patients in the radical group underwent distal gastric resection, whereas 86% of the patients in the standard group underwent pylorus preservation. The mean operative time in the radical group was 6.8 hours, compared with 6.2 hours in the standard group. There were no significant differences between the two groups with respect to the intraoperative blood loss, transfusion requirements, location of primary tumor, mean tumor size, positive lymph node status, or positive margin status. There were three deaths in the standard group and two in the radical group. The complication rates were 34% for the standard group and 40% for the radical group. Patients undergoing radical resection had a higher incidence of early delayed gastric emptying but had similar rates of other complications, such as pancreatic fistula, wound infection, intraabdominal abscess, and need for reoperation. The mean total number of lymph nodes resected was higher in the radical group. Of the 58 patients in the radical group, only 10% had metastatic carcinoma in the resected retroperitoneal lymph nodes, and none of those patients had the retroperitoneal nodes as the only site of lymph node involvement. The 1-year actuarial survival rate for patients surviving the immediate postoperative periods was 77% for the standard resection group and 83% for the radical resection group.
Conclusions: These data demonstrate that radical pancreaticoduodenectomy (with the addition of a distal gastrectomy and extended retroperitoneal lymphadenectomy to a standard pancreaticoduodenectomy) can be performed with similar morbidity and mortality to standard pancreaticoduodenectomy. However, the survival data are not sufficiently mature and the numbers of patients enrolled are not adequate to allow firm conclusions to be drawn regarding survival benefit.
Figures
Comment in
-
Does prophylactic octreotide decrease the rates of pancreatic fistula and other complications after pancreaticoduodenectomy?Ann Surg. 2001 Aug;234(2):262-3. doi: 10.1097/00000658-200108000-00017. Ann Surg. 2001. PMID: 11505073 Free PMC article. No abstract available.
References
-
- Geer RJ, Brennan MF. Prognostic indicators for survival after resection of pancreatic adenocarcinoma. Am J Surg 1993; 165: 68–73. - PubMed
-
- Delcore R, Rodriquez FJ, Forster J, et al. Significance of lymph node metastases in patients with pancreatic cancer undergoing curative resection. Am J Surg 1996; 172: 463–469. - PubMed
-
- Sohn TA, Lillemoe KD, Cameron JL, et al. Adenocarcinoma of the duodenum: factors influencing long-term survival. J Gastrointest Surg 1998; 2: 79–87. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
