

Gastric surgery for pseudotumor cerebri associated with severe obesity
- PMID: 10235521
- PMCID: PMC1420807
- DOI: 10.1097/00000658-199905000-00005
Gastric surgery for pseudotumor cerebri associated with severe obesity
Abstract
Objective: To study the efficacy of gastric surgery-induced weight loss for the treatment of pseudotumor cerebri (PTC).
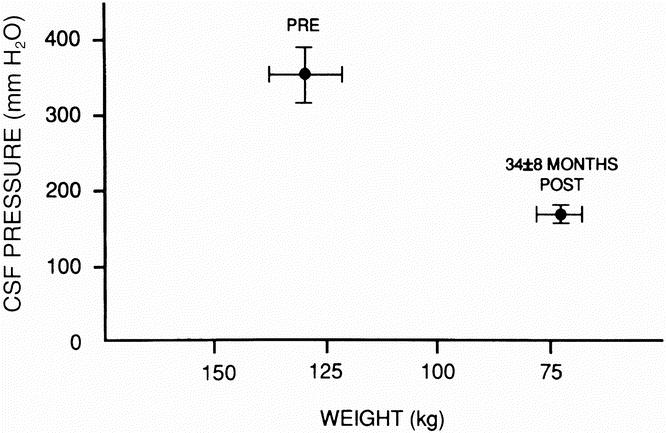
Summary background data: Pseudotumor cerebri (also called idiopathic intracranial hypertension), a known complication of severe obesity, is associated with severe headaches, pulsatile tinnitus, elevated cerebrospinal fluid (CSF) pressures, and normal brain imaging. The authors have found in previous clinical and animal studies that PTC in obese persons is probably secondary to a chronic increase in intraabdominal pressure leading to increased intrathoracic pressure. CSF-peritoneal shunts have a high failure rate, probably because they involve shunting from a high-pressure system to another high-pressure zone. In an earlier study of gastric bypass surgery in eight patients, CSF pressure decreased from 353+/-35 to 168+/-12 mm H2O at 34+/-8 months after surgery, with resolution of headaches in all.
Methods: Twenty-four severely obese women underwent bariatric surgery--23 gastric bypasses and one laparoscopic adjustable gastric banding--62+/-52 months ago for the control of severe obesity associated with PTC. CSF pressures were 324+/-83 mm H2O. Additional PTC central nervous system and cranial nerve problems included peripheral visual field loss, trigeminal neuralgia, recurrent Bell's palsy, and pulsatile tinnitus. Spontaneous CSF rhinorrhea occurred in one patient, and hemiplegia with homonymous hemianopsia developed as a complication of ventriculoperitoneal shunt placement in another. There were two occluded lumboperitoneal shunts and another functional but ineffective lumboperitoneal shunt. Additional obesity comorbidity in these patients included degenerative joint disease, gastroesophageal reflux disease, hypertension, urinary stress incontinence, sleep apnea, obesity hypoventilation, and type II diabetes mellitus.
Results: At 1 year after bariatric surgery, 19 patients lost an average of 45+/-12 kg, which was 71+/-18% of their excess weight. Their body mass index and percentage of ideal body weight had fallen to 30+/-5 kg/m2 and 133+/-22%, respectively. In four patients, less than 1 year had elapsed since surgery. Five patients were lost to follow-up. Surgically induced weight loss was associated with resolution of headache and pulsatile tinnitus in all but one patient within 4 months of the procedure. The cranial nerve dysfunctions resolved in all patients. The patient with CSF rhinorrhea had resolution within 4 weeks of gastric bypass. Of the 19 patients not lost to follow-up, 2 regained weight, with recurrence of headache and pulsatile tinnitus. Additional resolved associated comorbidities were 6/14 degenerative joint disease, 9/10 gastroesophageal reflux disorder, 2/6 hypertension, and all with sleep apnea, hypoventilation, type II diabetes mellitus, and urinary incontinence.
Conclusions: Bariatric surgery is the long-term procedure of choice for severely obese patients with PTC and is shown to have a much higher rate of success than CSF-peritoneal shunting reported in the literature, as well as providing resolution of additional obesity comorbidity. Increased intraabdominal pressure associated with central obesity is the probable etiology of PTC, a condition that should no longer be considered idiopathic.
Figures
References
-
- Newborg B. Pseudotumor cerebri treated by rice-reduction diet. Arch Intern Med 1974; 133: 802–807. - PubMed
-
- Amaral JF, Tsiaris W, Morgan T, Thompson WR. Reversal of benign intracranial hypertension by surgically induced weight loss. Arch Surg 1987; 122: 946–949. - PubMed
-
- Noggle JD, Rodning CB. Rapidly advancing pseudotumor cerebri associated with morbid obesity: an indication for gastric exclusion. South Med J 1986; 79: 761–763. - PubMed
-
- Sugerman HJ, Felton WL III, Salvant JB Jr, et al. Effects of surgically induced weight loss on idiopathic intracranial hypertension in morbid obesity. Neurology 1995; 45: 1655–1659. - PubMed
-
- Sismanis A, Butts FM, Hughes GB. Objective tinnitus in benign intracranial hypertension: an update. Laryngoscope 1990; 100: 331–336. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
