

18Fluorodeoxyglucose-positron emission tomography in the management of patients with suspected pancreatic cancer
- PMID: 10235532
- PMCID: PMC1420818
- DOI: 10.1097/00000658-199905000-00016
18Fluorodeoxyglucose-positron emission tomography in the management of patients with suspected pancreatic cancer
Abstract
Objective: To assess the accuracy and clinical impact of 18fluorodeoxyglucose-positron emission tomography (18FDG-PET) on the management of patients with suspected primary or recurrent pancreatic adenocarcinoma, and to assess the utility of 18FDG-PET in grading tumor response to neoadjuvant chemoradiation.
Summary background data: The diagnosis, staging, and treatment of pancreatic cancer remain difficult. Small primary tumors and hepatic metastases are often not well visualized by computed tomographic scanning (CT), resulting in a high incidence of nontherapeutic celiotomy and the frequent need for "blind resection." In addition, the distinction between local recurrence and nonspecific postoperative changes after resection can be difficult to ascertain on standard anatomic imaging. 18FDG-PET is a new imaging technique that takes advantage of increased glucose metabolism by tumor cells and may improve the diagnostic accuracy of preoperative studies for pancreatic adenocarcinoma.
Methods: Eighty-one 18FDG-PET scans were obtained in 70 patients undergoing evaluation for suspected primary or recurrent pancreatic adenocarcinoma. Of this group, 65 underwent evaluation for suspected primary pancreatic cancer. Nine patients underwent 18FDG-PET imaging before and after neoadjuvant chemoradiation, and in eight patients 18FDG-PET scans were performed for possible recurrent adenocarcinoma after resection. The 18FDG-PET images were analyzed visually and semiquantitatively using the standard uptake ratio (SUR). The sensitivity and specificity of 18FDG-PET and CT were determined for evaluation of the preoperative diagnosis of primary pancreatic carcinoma, and the impact of 18FDG-PET on patient management was retrospectively assessed.
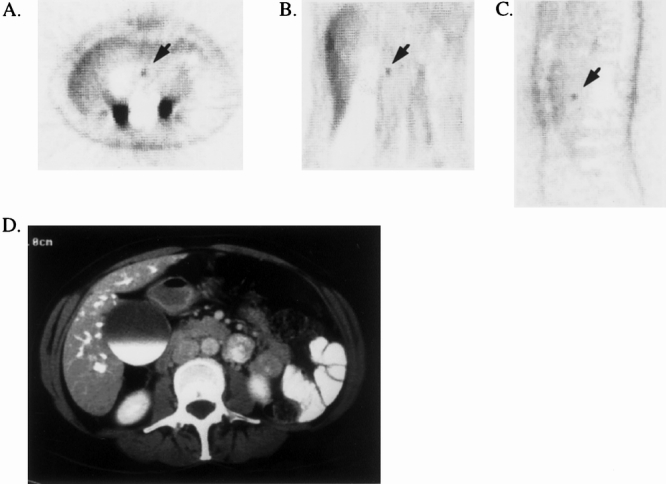
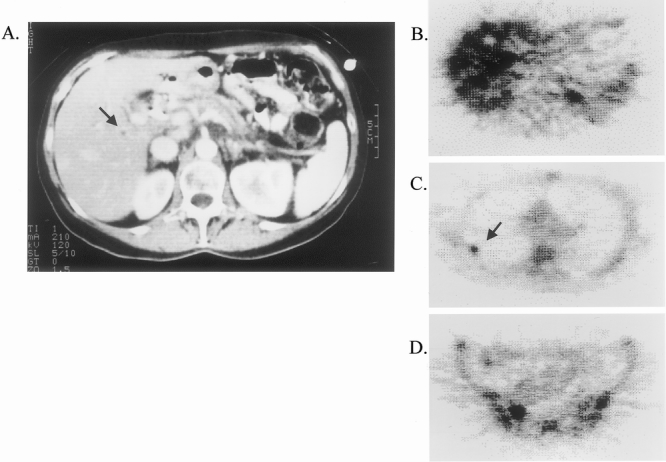
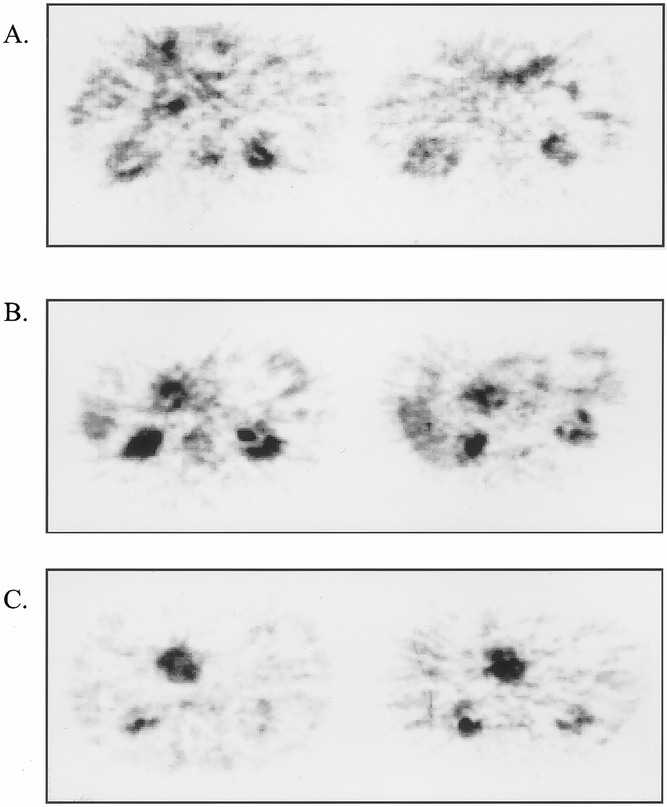
Results: Among the 65 patients evaluated for primary tumor, 52 had proven pancreatic adenocarcinoma and 13 had benign lesions. 18FDG-PET had a higher sensitivity and specificity than CT in correctly diagnosing pancreatic carcinoma (92% and 85% vs. 65% and 62%). Eighteen patients (28%) had indeterminate or unrecognized pancreatic masses on CT clarified with 18FDG-PET. Seven patients (11%) had indeterminate or unrecognized metastatic disease clarified with 18FDG-PET. Overall, 18FDG-PET suggested potential alterations in clinical management in 28/65 patients (43%) with suspected primary pancreatic adenocarcinoma. Of the nine patients undergoing 18FDG-PET imaging before and after neoadjuvant chemoradiation, four had evidence of tumor regression by PET, three showed stable disease, and two showed tumor progression. CT was unable to detect any response to neoadjuvant therapy in this group. Eight patients had 18FDG-PET scans to evaluate suspected recurrent disease after resection. Four were noted to have new regions of 18FDG-uptake in the resection bed; four had evidence of new hepatic metastases. All proved to have metastatic pancreatic adenocarcinoma.
Conclusions: These data confirm that 18FDG-PET is useful in the evaluation of patients with suspected primary or recurrent pancreatic carcinoma. 18FDG-PET is more sensitive and specific than CT in the detection of small primary tumors and in the clarification of hepatic and distant metastases. 18FDG-PET was also of benefit in assessing response to neoadjuvant chemoradiation. Although 18FDG-PET cannot replace CT in defining local tumor resectability, the application of 18FDG-PET in addition to CT may alter clinical management in a significant fraction of patients with suspected pancreatic cancer.
Figures
References
-
- McGuire GE, Pitt HA, Lillemoe KD, et al. Reoperative surgery for periampullary adenocarcinoma. Arch Surg 1991; 126: 1205–1212. - PubMed
-
- Robinson EK, Lee JE, Lowy AM, et al. Reoperative pancreaticoduodenectomy for periampullary carcinoma. Am J Surg 1996; 172: 432–438. - PubMed
-
- Thompson JS, Murayama KM, Edney JA, Rikkers LF. Pancreaticoduodenectomy for suspected but unproven malignancy. Am J Surg 1994; 169: 571–575. - PubMed
-
- Bouvet M, Bold R, Lee J, et al. Presumed malignant biliary obstruction despite a normal CT: data to support pancreaticoduodenectomy. Gastroenterology 1998; 114: S0033.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
