

Quantitative analysis of peristalsis in the guinea-pig small intestine using spatio-temporal maps
- PMID: 10332103
- PMCID: PMC2269346
- DOI: 10.1111/j.1469-7793.1999.0575t.x
Quantitative analysis of peristalsis in the guinea-pig small intestine using spatio-temporal maps
Abstract
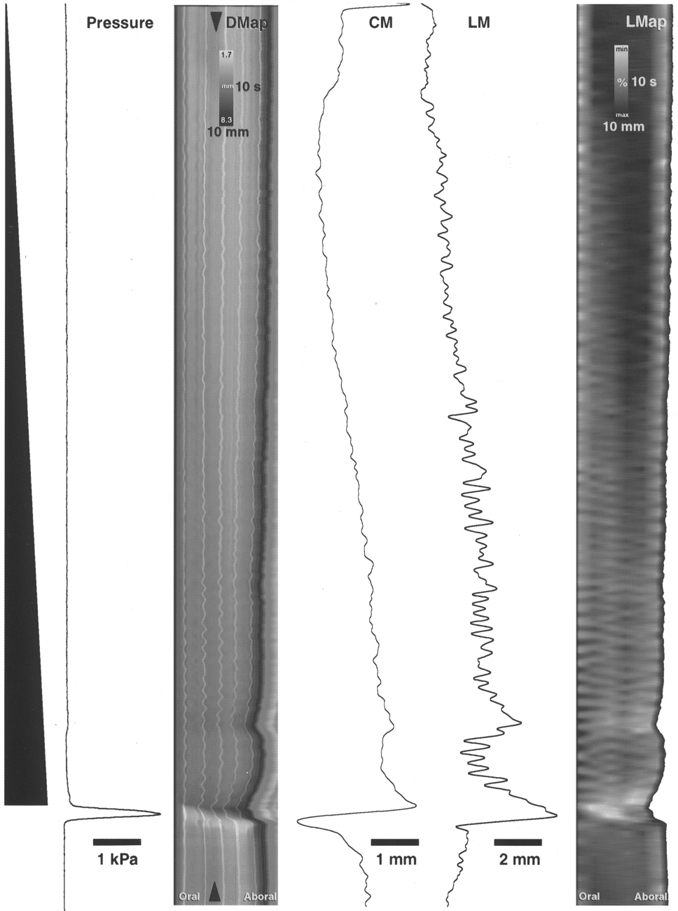
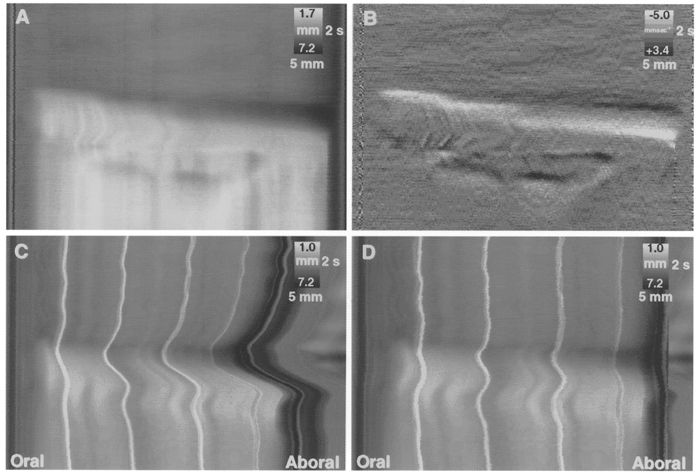
1. Peristalsis was evoked in guinea-pig small intestine by slow fluid infusion and recorded onto video and digitized. Spatio-temporal maps of diameter and longitudinal movement were constructed and parameters of motion were calculated. 2. During the filling of the isolated segments of intestine, rhythmic local longitudinal movements were observed at several points along the preparation. These phasic longitudinal muscle contractions were associated with small but significant local increases in diameter and probably reflect a passive mechanical coupling by connective tissue in the gut wall. In addition, occasional synchronized longitudinal muscle contractions caused net shortening of the preparation and always preceded the onset of peristaltic emptying. 3. Peristaltic emptying was characterized by a contraction of the circular muscle which usually started at the oral end of the preparation, that propagated aborally, propelling the contents. However, in 19 % of trials, the first circular muscle contraction occurred in the aboral half of the preparation. 4. The propagation of peristalsis consisted of separate sequential circular muscle contractions several centimetres long, particularly in the oral half of the preparation, giving a 'step-like' appearance to the spatio-temporal map. The gut was transiently distended aboral to the propagating circular muscle contraction due to the propulsion of contents. 5. At each point in the preparation, the longitudinal muscle remained contracted during the propulsive part of the circular muscle contraction. Only when the circular muscle contraction became lumen occlusive did lengthening of the longitudinal muscle take place. 6. Spatio-temporal maps are a powerful tool to visualize and analyse the complexity of gastrointestinal motility patterns.
Figures







References
-
- Alvarez WC, Zimmermann A. The absence of inhibition ahead of peristaltic rushes. American Journal of Physiology. 1927;83:52–59.
-
- Baur M. Die Peristaltik des isolierten Meerschweinchendunndarms im Filmversuch. Archives of Experimental Pathology and Pharmacology. 1928;133:69–83.
-
- Benard T, Bouchoucha M, Dupres M, Cugnenc PH. In vitro analysis of rat intestinal wall movements at rest and during propagated contraction - a new method. American Journal of Physiology. 1997;36:776–784. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources