

Influence of hospital and clinician workload on survival from colorectal cancer: cohort study
- PMID: 10334746
- PMCID: PMC27880
- DOI: 10.1136/bmj.318.7195.1381
Influence of hospital and clinician workload on survival from colorectal cancer: cohort study
Abstract
Objective: To determine whether clinician or hospital caseload affects mortality from colorectal cancer.
Design: Cohort study of cases ascertained between 1990 and 1994 by a region-wide colorectal cancer register.
Outcome measures: Mortality within a median follow up period of 54 months after diagnosis.
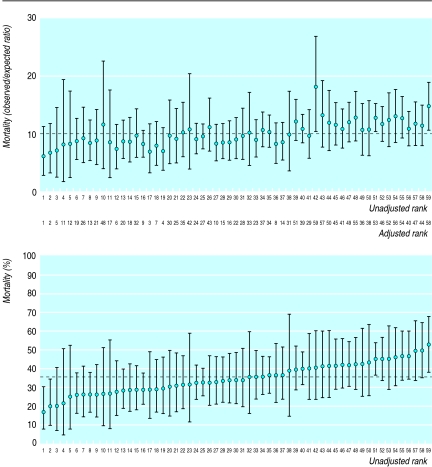
Results: Of the 3217 new patients registered over the period, 1512 (48%) died before 31 December 1996. Strong predictors of survival both in a logistic regression (fixed follow up) and in a Cox's proportional hazards model (variable follow up) were Duke's stage, the degree of tumour differentiation, whether the liver was deemed clear of cancer by the surgeon at operation, and the type of intervention (elective or emergency and curative or palliative intent). In a multilevel model, surgeon's caseload had no significant effect on mortality at 2 years. Hospital workload, however, had a significant impact on survival. The odds ratio for death within 2 years for cases managed in a hospital with a caseload of between 33 and 46 cases per year, 47 and 54 cases per year, and >/=55 cases per year (compared to one with </=23 cases per year) were respectively 1.48 (95% confidence interval 1.03 to 2.13), 1.52 (1.08 to 2.13), and 1.18 (0.83 to 1.68).
Conclusions: There was no detectable caseload effect for surgeons managing colorectal cancer, but survival of patients treated in hospitals with caseloads above 33 cases per year was slightly worse than for those treated in hospitals with fewer caseloads. Imprecise measurement of clinician specific "events rates" and the lack of routinely collected case mix data present major challenges for clinical audit and governance in the years ahead.
Figures
Comment in
-
Commentary: how experienced should a colorectal surgeon be?BMJ. 1999 May 22;318(7195):1386. BMJ. 1999. PMID: 10334747 No abstract available.
-
Some patients with colorectal cancer may have been missed by Northern Ireland registry.BMJ. 1999 Aug 7;319(7206):385. doi: 10.1136/bmj.319.7206.385a. BMJ. 1999. PMID: 10435979 Free PMC article. No abstract available.
-
Number of cases operated on is important in volume-outcome debate for colorectal cancer.BMJ. 1999 Aug 28;319(7209):576-7. BMJ. 1999. PMID: 10463912 Free PMC article. No abstract available.
References
-
- Expert Advisory Group on Cancer to the Chief Medical Officers of England and Wales. Consultative document: a policy framework for commissioning cancer services. London: Department of Health; 1994.
-
- Royal College of Surgeons of England and the Association of ColoProcology of Great Britain and Ireland. Guidelines for the management of colorectal cancer. London: RCSE and the Association of ColoProcology of Great Britain and Ireland; 1996.
-
- Department of Health. Guidance for purchasers. improving outcomes in colorectal cancer. The manual. London: DoH; 1997.
-
- NHS Centre for Reviews and Dissemination; University of York. The management of colorectal cancer. Effective Health Care. 1997;13:11–12.
-
- Taylor I. Debate: is volume important for outcome following surgery for common solid tumours? Eur J Surg Oncol. 1996;22:205–215.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical