

The influence of gatekeeping and utilization review on patient satisfaction
- PMID: 10337038
- PMCID: PMC1496580
- DOI: 10.1046/j.1525-1497.1999.00336.x
The influence of gatekeeping and utilization review on patient satisfaction
Abstract
Objective: To examine the influence of utilization review and denial of specialty referrals on patient satisfaction with overall medical care, willingness to recommend one's physician group to a friend, and desire to disenroll from the health plan.
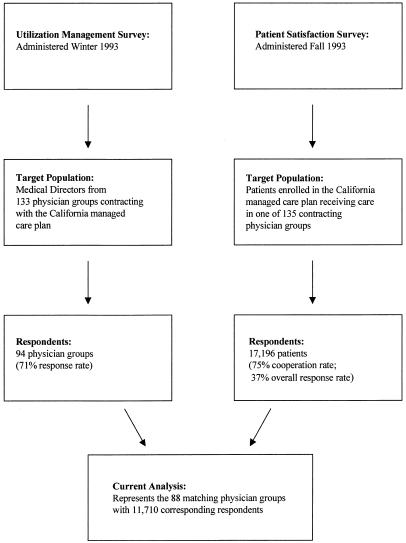
Design: Two cross-sectional questionnaires: one of physician groups and one of patient satisfaction.
Setting: Eighty-eight capitated physician groups in California.
Participants: Participants were 11,710 patients enrolled in a large California network-model HMO in 1993 who received care in one of the 88 physician groups.
Measurements and main results: Our main measures were how groups conducted utilization review for specialty referrals and tests, patient-reported denial of specialty referrals, and patient satisfaction with overall medical care. Patients in groups that required preauthorization for access to many types of specialists were significantly (p </=.001) less satisfied than patients in groups that had few preauthorization requirements, even after adjusting for patient and other group characteristics. Patients who had wanted to see a specialist in the previous year but did not see one were significantly less satisfied than those who had wanted to see a specialist and actually saw one (p <.001). In addition, patients who did not see a specialist when desired were more likely to want to disenroll from the health plan than patients who saw the specialist (40% vs 18%, p </=.001) and more likely not to recommend their group to a friend (38% vs 13%, p </=.001).
Conclusions: Policies that limited direct access to specialists, and especially denial of patient-desired referrals, were associated with significantly lower patient satisfaction, increased desire to disenroll, and lower likelihood of recommending the group to a friend. Health plans and physician groups need to take these factors into account when designing strategies to reduce specialty care use.
Figures
Comment in
-
The good (gatekeeper), the bad (gatekeeper), and the ugly (situation).J Gen Intern Med. 1999 May;14(5):320-1. doi: 10.1046/j.1525-1497.1999.00344.x. J Gen Intern Med. 1999. PMID: 10337044 Free PMC article. Review. No abstract available.
References
-
- Kassirer JP. Access to specialty care. N Engl J Med. 1994;331(17):1151–3. Editorial. - PubMed
-
- Greenfield S. Dividing up the turf: generalists versus specialists. J Gen Intern Med. 1996;11(4):245–6. - PubMed
-
- Mechanic D, Schlesinger M. The impact of managed care on patients’ trust in medical care and their physicians. JAMA. 1996;275(21):1693–7. - PubMed
-
- St. Peter RF. Gatekeeping Arrangements are in Wide-Spread Use. Results from the Community Tracking Study. Washington, DC: Center for Studying Health System Change; 1997(7). - PubMed
-
- Kerr EA, Mittman BS, Hays RD, Siu AL, Leake B, Brook RH. Managed care and capitation in California: how do physicians at financial risk control their own utilization? Ann Intern Med. 1995;123(7):500–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical