

Cytomegalovirus retinitis after the initiation of highly active antiretroviral therapy: a 2 year prospective study
- PMID: 10340970
- PMCID: PMC1723070
- DOI: 10.1136/bjo.83.6.652
Cytomegalovirus retinitis after the initiation of highly active antiretroviral therapy: a 2 year prospective study
Abstract
Background/aims: There have been several recent reports suggesting that the natural history of cytomegalovirus retinitis (CMVR) has been significantly modified with the development of highly active antiretroviral therapy (HAART). This 2 year prospective cohort study assesses the effect of HAART on the incidence and progression of CMV retinitis in patients with CD4 cell counts below 50 cells x10(6)/l.
Methods: 63 patients, with CD4 cell counts below 50 cells x10(6)/l, who were recruited to a 2 year prospective cohort study at the commencement of combination antiretroviral therapy including the use of the proteinase inhibitor, indinavir, were reported. The response to HAART was assessed in terms of a rise in the CD4 cell count and fall in HIV viral load. An experienced ophthalmologist performed dilated funduscopy at the time of recruitment and thereafter at 2 weekly intervals and retinal photography was performed at monthly intervals in patients with CMVR. The activity and progression of CMV retinitis was assessed on the basis of the characteristic clinical and photographic findings.
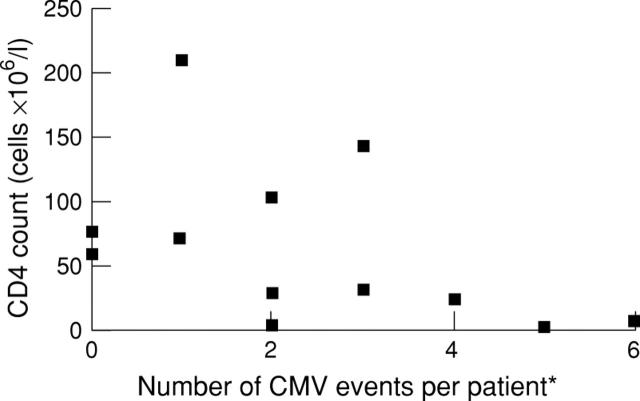
Results: 34 patients achieved at least 50 CD4 cells x10(6)/l at 3 months after initiation of therapy. New diagnoses of CMVR were seen only in the non-responder group (p=0. 085). Overall, the relative risk of a new retinitis event in this group was 3.52 (95% CI 1.16, 10.68) at 3 months compared with those patients who were responsive to HAART. 12 of the 63 patients had previous CMVR. Disease progression was associated with non-response to therapy (p=0.182 exact). In patients with CMVR the median time to first progression was 18 days (95% CI 8, 91) in non-responders and 121 days (95% CI 0.59, 3.65) in responders. By the end of the 2 year follow up period all surviving patients had >50 CD4 cells x10(6)/l. No CMV events were seen after 8 months of therapy in either group of patients.
Conclusions: These findings suggest that significant clinical immunorestoration to CMV occurs in response to HAART in patients with CMVR after a lag time of 3-8 months. Initially, a rise in CD4 count is predictive of CMVR response but after the lag period all survivors appear to have developed a clinical immunorestoration to CMV. If HAART is commenced in at risk patients before the development of CMVR the incidence of new disease falls significantly.
Figures
Similar articles
-
CMVR diagnoses and progression of CD4 cell counts and HIV viral load measurements in HIV patients on HAART.Br J Ophthalmol. 2001 Jul;85(7):837-41. doi: 10.1136/bjo.85.7.837. Br J Ophthalmol. 2001. PMID: 11423459 Free PMC article.
-
Influence of highly active antiretroviral therapy on the development of CMV disease in HIV positive patients at high risk for CMV disease.Br J Ophthalmol. 1999 Oct;83(10):1186-9. doi: 10.1136/bjo.83.10.1186. Br J Ophthalmol. 1999. PMID: 10502584 Free PMC article. Clinical Trial.
-
Effects of protease inhibitors on the course of CMV retinitis in relation to CD4+ lymphocyte responses in HIV+ patients.Br J Ophthalmol. 1998 Sep;82(9):988-90. doi: 10.1136/bjo.82.9.988. Br J Ophthalmol. 1998. PMID: 9893585 Free PMC article. Clinical Trial.
-
CMV retinitis and the controversies associated with highly active antiretroviral therapy and the immune recovery hypothesis.AIDS Patient Care STDS. 1998 Mar;12(3):181-5. doi: 10.1089/apc.1998.12.181. AIDS Patient Care STDS. 1998. PMID: 11361932 Review.
-
Changing patterns of HIV related ocular disease.Sex Transm Infect. 1999 Feb;75(1):18-20. doi: 10.1136/sti.75.1.18. Sex Transm Infect. 1999. PMID: 10448336 Free PMC article. Review.
Cited by
-
The incidence of cytomegalovirus (CMV) antigenemia and CMV disease is reduced by highly active antiretroviral therapy.Eur J Epidemiol. 2000 May;16(5):433-7. doi: 10.1023/a:1007619323939. Eur J Epidemiol. 2000. PMID: 10997830 Clinical Trial.
-
Suspension of anticytomegalovirus maintenance therapy following immune recovery due to highly active antiretroviral therapy.Br J Ophthalmol. 2001 Apr;85(4):471-3. doi: 10.1136/bjo.85.4.471. Br J Ophthalmol. 2001. PMID: 11264139 Free PMC article.
-
Long term visual outcome of patients with cytomegalovirus retinitis treated with highly active antiretroviral therapy.Br J Ophthalmol. 2003 Jul;87(7):853-5. doi: 10.1136/bjo.87.7.853. Br J Ophthalmol. 2003. PMID: 12812884 Free PMC article.
-
Ocular manifestations of acquired immunodeficiency syndrome in Korea.J Korean Med Sci. 2012 May;27(5):542-6. doi: 10.3346/jkms.2012.27.5.542. Epub 2012 Apr 25. J Korean Med Sci. 2012. PMID: 22563221 Free PMC article.
-
Cidofovir: a review of its use in cytomegalovirus retinitis in patients with AIDS.Drugs. 1999 Aug;58(2):325-45. doi: 10.2165/00003495-199958020-00015. Drugs. 1999. PMID: 10473024 Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials