

In vivo efficacies of combinations of beta-lactams, beta-lactamase inhibitors, and rifampin against Acinetobacter baumannii in a mouse pneumonia model
- PMID: 10348761
- PMCID: PMC89287
- DOI: 10.1128/AAC.43.6.1406
In vivo efficacies of combinations of beta-lactams, beta-lactamase inhibitors, and rifampin against Acinetobacter baumannii in a mouse pneumonia model
Abstract
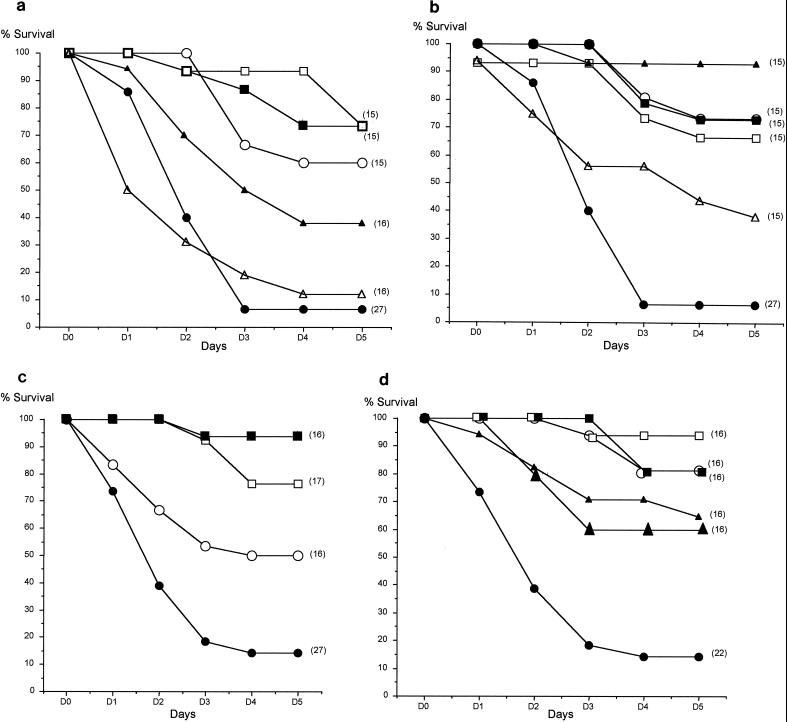
The effects of various regimens containing combinations of beta-lactams, beta-lactam inhibitor(s), and rifampin were assessed in a recently described mouse model of Acinetobacter baumannii pneumonia (M. L. Joly-Guillou, M. Wolff, J. J. Pocidalo, F. Walker, and C. Carbon, Antimicrob. Agents Chemother. 41:345-351, 1997). Two aspects of the therapeutic response were studied: the kinetics of the bactericidal effect (treatment was initiated 3 h after intratracheal inoculation, and bacterial counts were determined over a 24-h period) and survival (treatment was initiated 8 h after inoculation, and the cumulative mortality rate was assessed on day 5). Two clinical strains were used: a cephalosporinase-producing strain (SAN-94040) and a multiresistant strain (RCH-69). For SAN-94040 and RCH-69, MICs and MBCs (milligrams per liter) were as follows: ticarcillin, 32, 64, 256, and >256, respectively; ticarcillin-clavulanate, 32, 64, and 512, and >512, respectively; imipenem, 0.5, 0.5, 8, and 32, respectively; sulbactam, 0.5, 0.5, 8, and 8, respectively; and rifampin, 8, 8, 4, and 4, respectively. Against SAN-94040, four regimens, i.e., imipenem, sulbactam, imipenem-rifampin, and ticarcillin-clavulanate (at a 25/1 ratio)-sulbactam produced a true bactericidal effect (>/=3-log10 reduction of CFU/g of lung). The best survival rate (i.e., 93%) was obtained with the combination of ticarcillin-clavulanate-sulbactam, and regimens containing rifampin provided a survival rate of >/=65%. Against RCH-69, only regimens containing rifampin and the combination of imipenem-sulbactam had a true bactericidal effect. The best survival rates (>/=80%) were obtained with regimens containing rifampin and sulbactam. These results suggest that nonclassical combinations of beta-lactams, beta-lactamase inhibitors, and rifampin should be considered for the treatment of nosocomial pneumonia due to A. baumannii.
Figures
References
-
- Anstey N M, Curry B J, Withnall K M. Community-acquired Acinetobacter pneumonia in the northern territory of Australia. Clin Infect Dis. 1992;14:83–91. - PubMed
-
- Chang-Xiao L, Jia-Rong W, Yi-Li L. Pharmacokinetics of sulbactam and ampicillin in mice and in dogs. Eur J Pharmacol. 1990;183:1859–1860.
-
- Corbella X, Ariza J, Ardanuy C, Vuelta M, Tubeau F, Sora M, Pujol M, Gudiol F. Efficacy of sulbactam alone and in combination with ampicillin in nosocomial infections caused by multiresistant Acinetobacter baumannii. J Antimicrob Chemother. 1998;42:793–802. - PubMed
-
- Costa S F, Wodcock J, Child J, Caiaffa H H, Gill M, Wise R, Levin A S. Abstracts of the 36th Interscience Conference on Antimicrobial Agents and Chemotherapy. Washington, D.C: American Society for Microbiology; 1996. Characterization of the β-lactamase and outer-membrane proteins of imipenem-resistant Acinetobacter baumannii clinical isolates from Brazil, abstr. C123; p. 56.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
