

Vancomycin-resistant enterococci in intensive-care hospital settings: transmission dynamics, persistence, and the impact of infection control programs
- PMID: 10359812
- PMCID: PMC22015
- DOI: 10.1073/pnas.96.12.6908
Vancomycin-resistant enterococci in intensive-care hospital settings: transmission dynamics, persistence, and the impact of infection control programs
Abstract
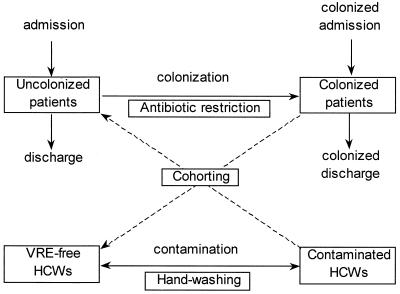
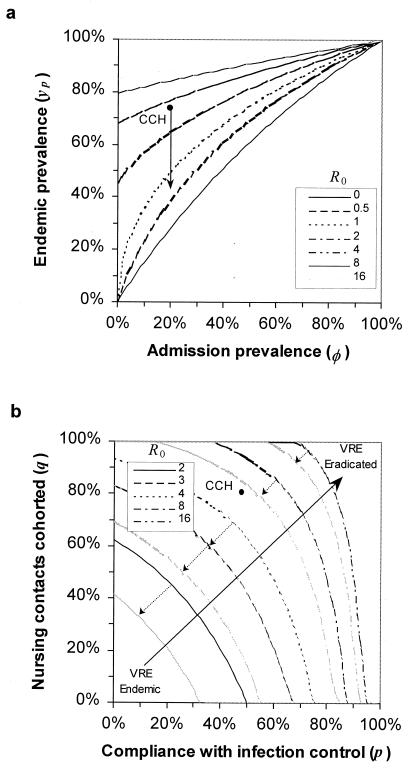
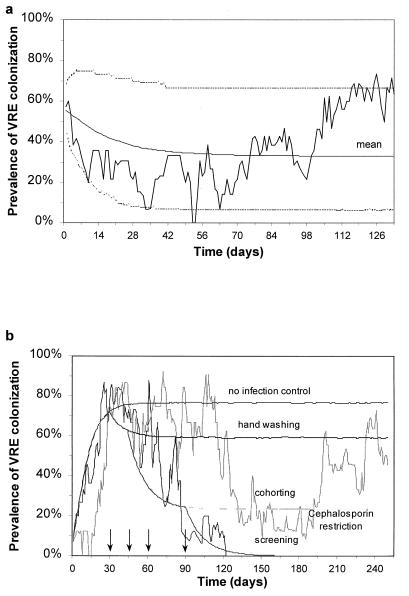
Vancomycin-resistant enterococci (VRE) recently have emerged as a nosocomial pathogen especially in intensive-care units (ICUs) worldwide. Transmission via the hands of health-care workers is an important determinant of spread and persistence in a VRE-endemic ICU. We describe the transmission of nosocomial pathogens by using a micro-epidemiological framework based on the transmission dynamics of vector-borne diseases. By using the concept of a basic reproductive number, R0, defined as the average number of secondary cases generated by one primary case, we show quantitatively how infection control measures such as hand washing, cohorting, and antibiotic restriction affect nosocomial cross-transmission. By using detailed molecular epidemiological surveillance and compliance monitoring, we found that the estimated basic reproductive number for VRE during a study at the Cook County Hospital, Chicago, was approximately 3-4 without infection control and 0.7 when infection control measures were included. The impact of infection control was to reduce the prevalence from a predicted 79% to an observed 36%. Hand washing and staff cohorting are the most powerful control measures although their efficacy depends on the magnitude of R0. Under the circumstances tested, endemicity of VRE was stabilized despite infection control measures, by the constant introduction of colonized patients. Multiple stochastic simulations of the model revealed excellent agreement with observed pattern. In conjunction with detailed microbiological surveillance, a mathematical framework provides a precise template to describe the colonization dynamics of VRE in ICUs and impact of infection control measures. Our analyses suggest that compliance for hand washing significantly in excess of reported levels, or the cohorting of nursing staff, are needed to prevent nosocomial transmission of VRE in endemic settings.
Figures
References
-
- Centre for Disease Control. Morbid Mortal Wkly Rep. 1995;44:1–13.
-
- Public Health Laboratory Service. CDR Weekly. 1996;6:1.
-
- Palmer S M, Rybak M J. Pharmacotherapy. 1996;16:819–829. - PubMed
-
- Husani R, Raad I. Curr Opin Intensive Care. 1997;10:431–434.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
