

Remitting seronegative symmetrical synovitis with pitting oedema (RS3PE) syndrome: a prospective follow up and magnetic resonance imaging study
- PMID: 10364902
- PMCID: PMC1752869
- DOI: 10.1136/ard.58.4.230
Remitting seronegative symmetrical synovitis with pitting oedema (RS3PE) syndrome: a prospective follow up and magnetic resonance imaging study
Abstract
Objective: To determine the clinical characteristics of patients with "pure" remitting seronegative symmetrical synovitis with pitting oedema (RS3PE) syndrome, and to investigate its relation with polymyalgia rheumatica (PMR). Magnetic resonance imaging (MRI) was used to describe the anatomical structures affected by inflammation in pure RS3PE syndrome.
Methods: A prospective follow up study of 23 consecutive patients with pure RS3PE syndrome and 177 consecutive patients with PMR diagnosed over a five year period in two Italian secondary referral centres of rheumatology. Hands or feet MRI, or both, was performed at diagnosis in 7 of 23 patients.
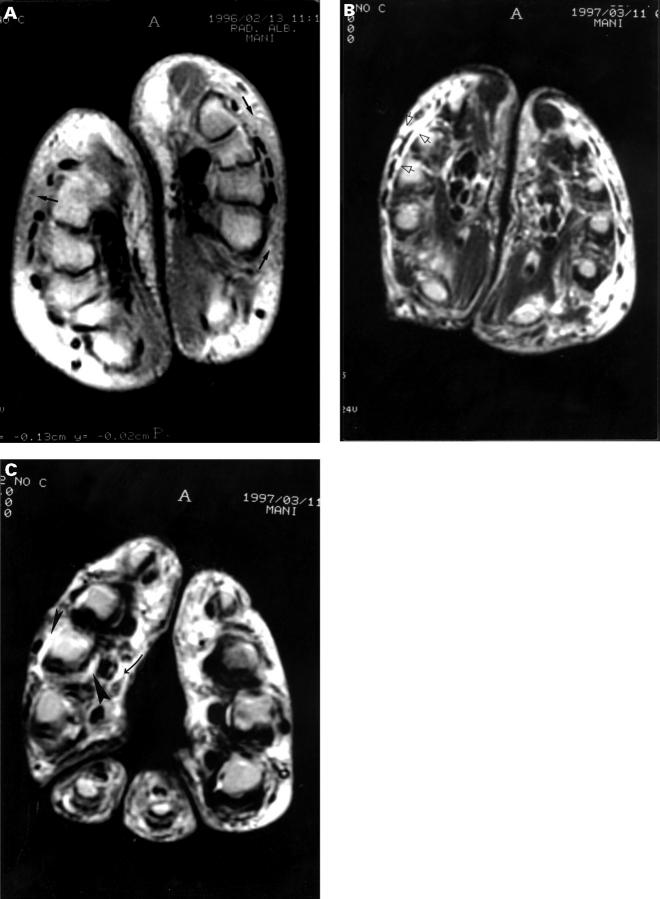
Results: At inspection evidence of hand and/or foot tenosynovitis was present in all the 23 patients with pure RS3PE syndrome. Twenty one (12%) patients with PMR associated distal extremity swelling with pitting oedema. No significant differences in the sex, age at onset of disease, acute phase reactant values at diagnosis, frequency of peripheral synovitis and carpal tunnel syndrome and frequency of HLA-B7 antigen were present between patients with pure RS3PE and PMR. In both conditions no patient under 50 was observed, the disease frequency increased significantly with age and the highest frequency was present in the age group 70-79 years. Clinical symptoms for both conditions responded promptly to corticosteroids and no patient developed rheumatoid arthritis during the follow up. However, the patients with pure RS3PE syndrome were characterised by shorter duration of treatment, lower cumulative corticosteroid dose and lower frequency of systemic signs/symptoms and relapse/recurrence. Hands and feet MRI showed evidence of tenosynovitis in five patients and joint synovitis in three patients.
Conclusion: The similarities of demographic, clinical, and MRI findings between RS3PE syndrome and PMR and the concurrence of the two syndromes suggest that these conditions may be part of the same disease and that the diagnostic labels of PMR and RS3PE syndrome may not indicate a real difference. The presence of distal oedema seems to indicate a better prognosis.
Figures

Comment in
-
RS3PE: six years later.Ann Rheum Dis. 1999 Nov;58(11):722-3. doi: 10.1136/ard.58.11.722. Ann Rheum Dis. 1999. PMID: 10610676 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
