

Case Reports
Idiopathic spinal cord herniation: value of MR phase-contrast imaging
Affiliations
- PMID: 10369369
- PMCID: PMC7056135
Item in Clipboard
Case Reports
Idiopathic spinal cord herniation: value of MR phase-contrast imaging
AJNR Am J Neuroradiol.
1999 May.
Abstract
We report two patients with an idiopathic transdural spinal cord herniation at the thoracic level. Phase-contrast MR imaging was helpful in showing an absence of CSF flow ventral to the herniated cord and a normal CSF flow pattern dorsal to the cord, which excluded a compressive posterior arachnoid cyst.
Figures
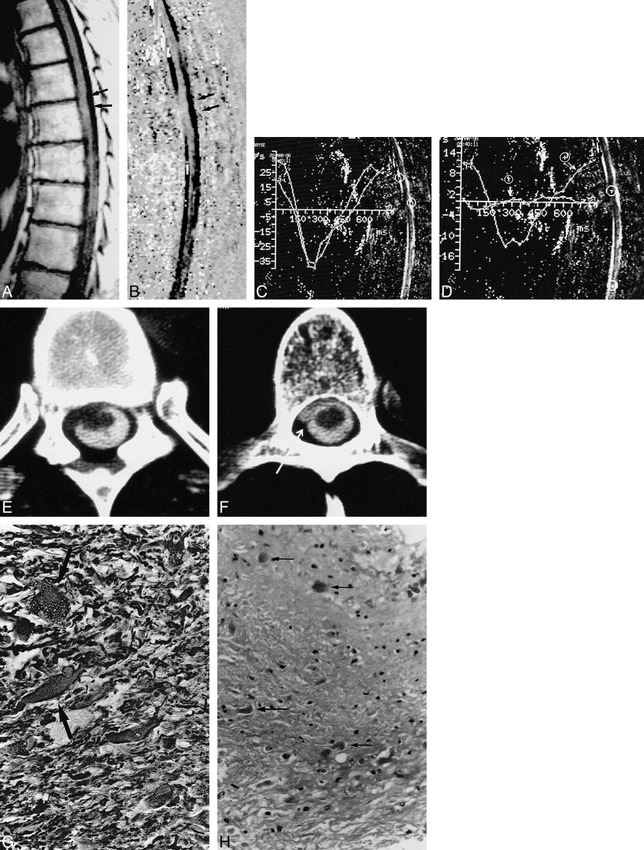
Case 1: spontaneous spinal cord herniation. A, Sagittal T1-weighted MR image shows ventral displacement of the spinal cord at the T6 level (arrows). B, Sagittal velocity image during systolic phase, 300 milliseconds after the R wave of the EKG. Dark areas correspond to craniocaudal flow. No flow is visible on the ventral side of the spinal cord at the T6 level. Normal flow is seen in the posterior subarachnoid spaces. A posterior arachnoid cyst is unlikely. C and D, Evolution of CSF flow during the RR cycle of the ECG. By convention, caudal flow is represented as negative. CSF velocity curves measured in the anterior subarachnoid spaces superior to the cord herniation and in the posterior subarachnoid spaces at the level of the herniation show similar normal patterns (C). There is no evidence of an associated posterior arachnoid cyst. Cursors have been placed at the level of the herniation (T) and below it (+). There is limited cord motion at the level of the herniation, as manifested by a minimal deflection of the pulse wave, T, from zero, whereas normal cord motion is identified below the herniation (D). E and F, CT myelography at the level of the cord herniation (E): the cord is ventrally displaced and protrudes into the left anterolateral epidural space. Just below the cord herniation, an anterior pseudomeningocele is filled with contrast medium (arrow, F). G, On histopathologic section, hypertrophic astrocytes are visible in some areas (arrows) (alkaline phosphatase-antialkaline phosphatase method for GFAP, original magnification ×400). H, Histologic section shows chronic reactive changes with Rosenthal fibers (arrows) and mild pilocytic gliosis (H and E, original magnification ×250).
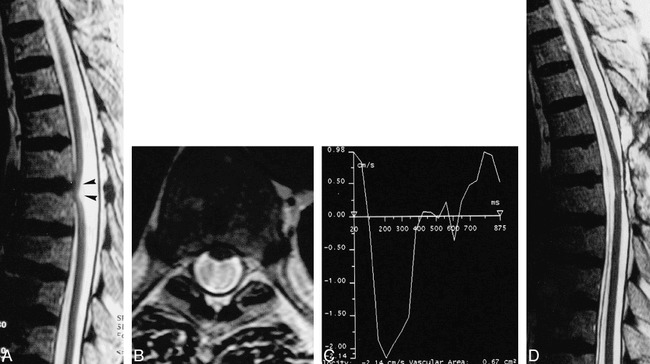
Case 2: ISCH. A, Sagittal T2-weighted MR image shows ventral displacement of the spinal cord at the T5–T6 level (arrowheads). B, Axial T2-weighted MR image at the level of the cord herniation shows anterior cord displacement and loss of the anterior subarachnoid spaces. Loss of phase coherence is responsible for the dark signal in the dorsal subarachnoid space. C, CSF velocity curve measured in the posterior subarachnoid spaces at the level of the herniation shows a normal CSF velocity pattern. A posterior arachnoid cyst was considered unlikely. D, Postoperative sagittal T2-weighted MR image shows normal location of the spinal cord.
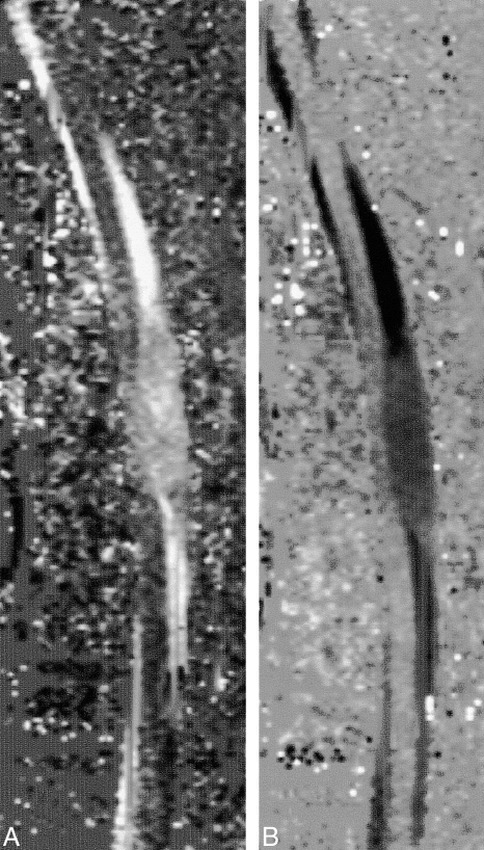
Arachnoid cyst. A and B, Sagittal velocity images during diastolic (A) and systolic (B) phases show low CSF flow (gray areas). The contents of the distended arachnoid cyst are clearly visible along the dorsal side of the spinal cord.
Similar articles
-
Spontaneous thoracic spinal cord herniation.Neurology. 2004 Dec 14;63(11):2187. doi: 10.1212/01.wnl.0000140620.32658.0b. Neurology. 2004. PMID: 15596780 No abstract available.
-
Idiopatic spinal cord herniation: a treatable cause of Brown-Séquard syndrome.Acta Neurochir (Wien). 2002 Apr;144(4):321-5. doi: 10.1007/s007010200044. Acta Neurochir (Wien). 2002. PMID: 12021877
-
Idiopathic spinal cord herniation: a treatable cause of the Brown-Sequard syndrome--case report.Neurosurgery. 1995 May;36(5):1028-32; discussion 1032-3. doi: 10.1227/00006123-199505000-00023. Neurosurgery. 1995. PMID: 7791969
-
Idiopathic spinal cord herniation. Report of two cases and review of the literature.J Neurosurg. 1998 Feb;88(2):331-5. doi: 10.3171/jns.1998.88.2.0331. J Neurosurg. 1998. PMID: 9452246 Review.
-
Spontaneous thoracic spinal cord herniation. A case report.Spine (Phila Pa 1976). 1996 Jul 15;21(14):1710-3. doi: 10.1097/00007632-199607150-00019. Spine (Phila Pa 1976). 1996. PMID: 8839477 Review.
Cited by
-
Idiopathic thoracic spinal cord herniation: retrospective analysis supporting a mechanism of diskogenic dural injury and subsequent tamponade.AJNR Am J Neuroradiol. 2012 Jan;33(1):52-6. doi: 10.3174/ajnr.A2730. Epub 2011 Dec 8. AJNR Am J Neuroradiol. 2012. PMID: 22158920 Free PMC article. Review.
-
Understanding Idiopathic Spinal Cord Herniation - A Comprehensive Review of Imaging and Literature.J Clin Imaging Sci. 2019 May 24;9:22. doi: 10.25259/JCIS-25-2019. eCollection 2019. J Clin Imaging Sci. 2019. PMID: 31448173 Free PMC article.
-
Idiopathic Spinal Cord Herniation Associated With a Thoracic Disc Herniation: Case Report, Surgical Video, and Literature Review.Clin Spine Surg. 2020 Jul;33(6):222-229. doi: 10.1097/BSD.0000000000000896. Clin Spine Surg. 2020. PMID: 32101990 Free PMC article. Review.
-
The Pathogenesis of Ventral Idiopathic Herniation of the Spinal Cord: A Hypothesis Based on the Review of the Literature.Front Neurol. 2017 Sep 11;8:476. doi: 10.3389/fneur.2017.00476. eCollection 2017. Front Neurol. 2017. PMID: 28955299 Free PMC article.
-
Idiopathic spinal cord herniation: Clinical review and report of three cases.Asian J Neurosurg. 2013 Apr;8(2):97-105. doi: 10.4103/1793-5482.116386. Asian J Neurosurg. 2013. PMID: 24049553 Free PMC article. Review.
References
-
- Baur A, Stabler A, Psenner K,, et al. Imaging findings in patients with ventral dural defects and herniation of neural tissue. Eur Radiol 1997;7:1259-1263 - PubMed
-
- Borges LF, Zervas NT, Lehrich JR. Idiopathic spinal cord herniation: a treatable cause of the Brown-Sequard syndrome. Neurosurgery 1995;36:1028-1033 - PubMed
-
- Hausmann ON, Moseley IF. Idiopathic dural herniation of the thoracic spinal cord. Neuroradiology 1996;38:503-510 - PubMed
-
- Isu T, Iizuka T, Iwasaki Y,, et al. Spinal cord herniation associated with an intradural spinal arachnoid cyst diagnosed by magnetic resonance imaging. Neurosurgery 1991;29:137-139 - PubMed
-
- Kumar R, Taha J, Greiner AL. Herniation of the spinal cord: case report. J Neurosurg 1995;82:131-136 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical