

Microchimerism of maternal origin persists into adult life
- PMID: 10393697
- PMCID: PMC408407
- DOI: 10.1172/JCI6611
Microchimerism of maternal origin persists into adult life
Abstract
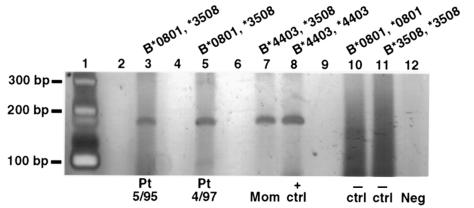
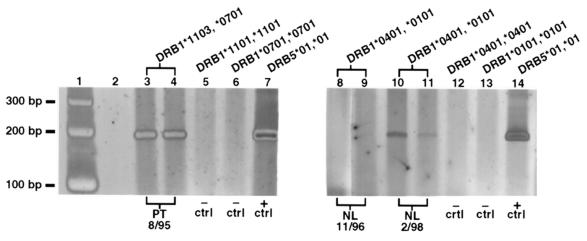
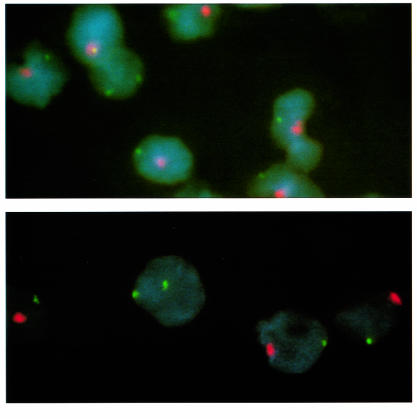
Recent studies indicate that fetal cells persist in maternal blood for decades after pregnancy. Maternal cells are known to engraft and persist in infants with immunodeficiency, but whether maternal cells persist long-term in immunocompetent offspring has not specifically been investigated. We developed sensitive human leukocyte antigen-specific (HLA-specific) PCR assays and targeted nonshared maternal HLA genes to test for persistent maternal microchimerism in subjects with scleroderma and in healthy normal subjects. Nonshared maternal-specific DNA was found in 6 of 9 scleroderma patients. In situ hybridization with double labeling for X and Y chromosome-specific sequences revealed female cells in peripheral blood samples from 2 male scleroderma patients. HLA-specific PCR also frequently revealed persistent maternal microchimerism in healthy control subjects. The mean age of all subjects with maternal microchimerism was 28 years (range: 9-49 years). With few exceptions, mothers of subjects with persistent maternal microchimerism were HLA incompatible with subjects for class I and class II alleles. These results clearly indicate that HLA-disparate maternal cells can persist in immunocompetent offspring well into adult life. The biological significance of maternal microchimerism and whether it might contribute to autoimmune disease requires further investigation.
Figures
References
-
- Lo YMD, et al. Two-way cell traffic between mother and fetus: biologic and clinical implications. Blood. 1996;88:4390–4395. - PubMed
-
- Hall JM, et al. Detection of maternal cells in human umbilical cord blood using fluorescence in situ hybridization. Blood. 1995;86:2829–2832. - PubMed
-
- Pollack MS, Kirpatrick D, Kapoor D, Supor V, O’Reilly RJ. Identification by HLA typing of intrauterine derived maternal T cells in four patients with severe combined immunodeficiency. N Engl J Med. 1982;307:662–666. - PubMed
-
- Nelson JL. Viewpoint. Maternal-fetal immunology and autoimmune disease. Is some autoimmune disease auto-alloimmune or allo-autoimmune? Arthritis Rheum. 1996;39:191–194. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
