

Injection of pre-psoriatic skin with CD4+ T cells induces psoriasis
- PMID: 10393847
- PMCID: PMC1866658
- DOI: 10.1016/S0002-9440(10)65109-7
Injection of pre-psoriatic skin with CD4+ T cells induces psoriasis
Abstract
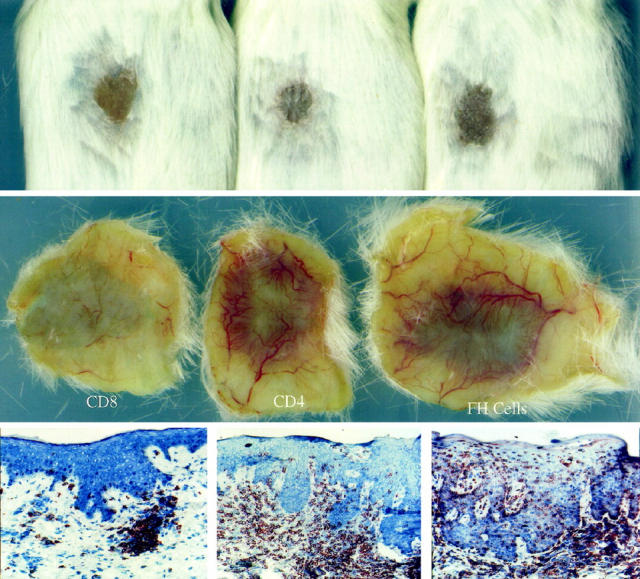
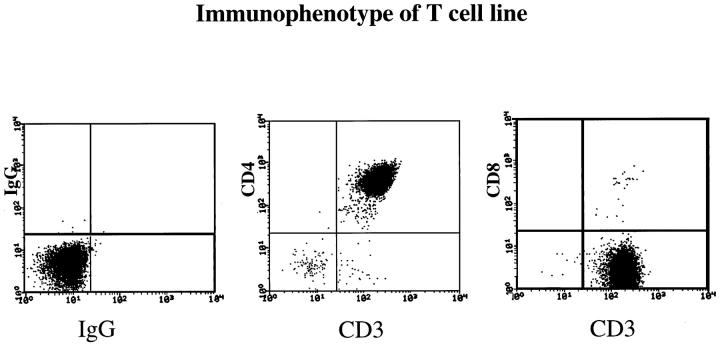
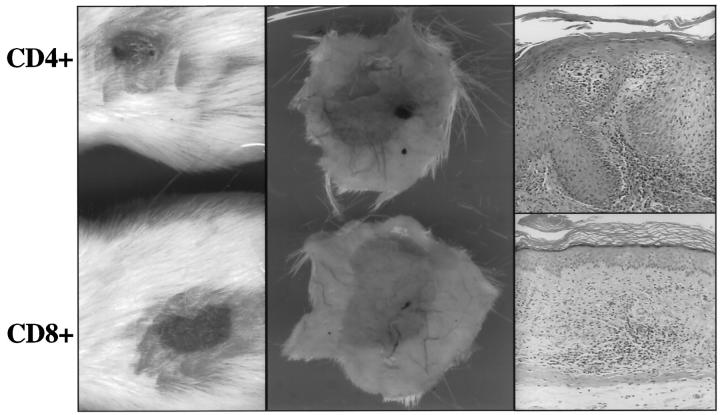
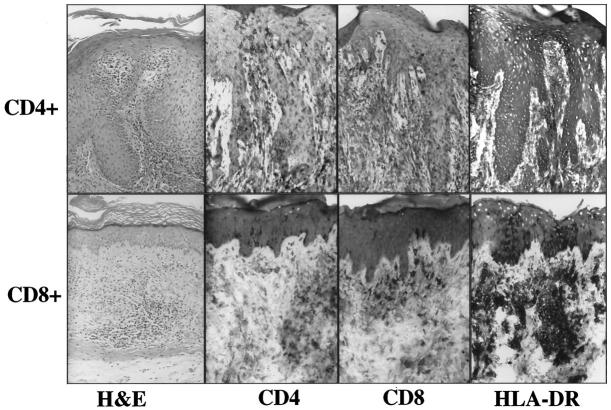
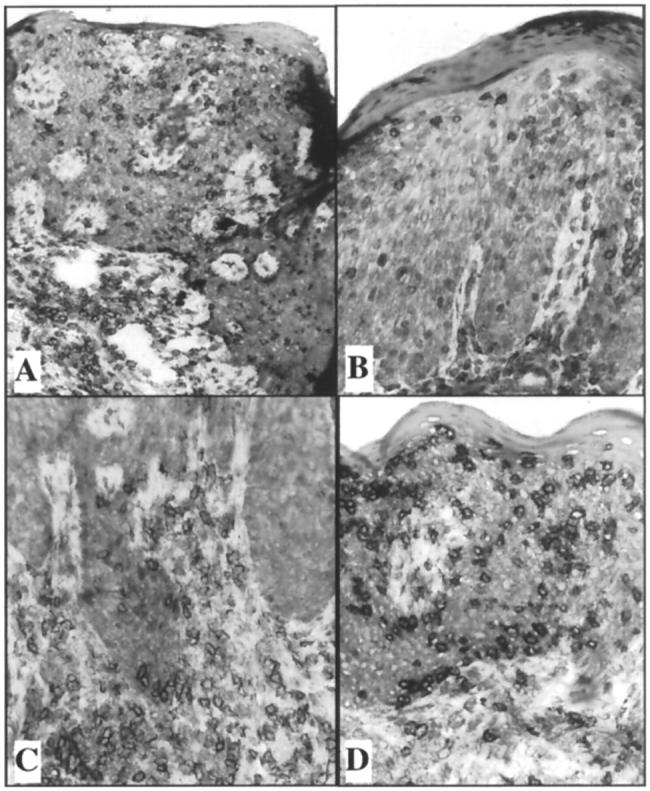
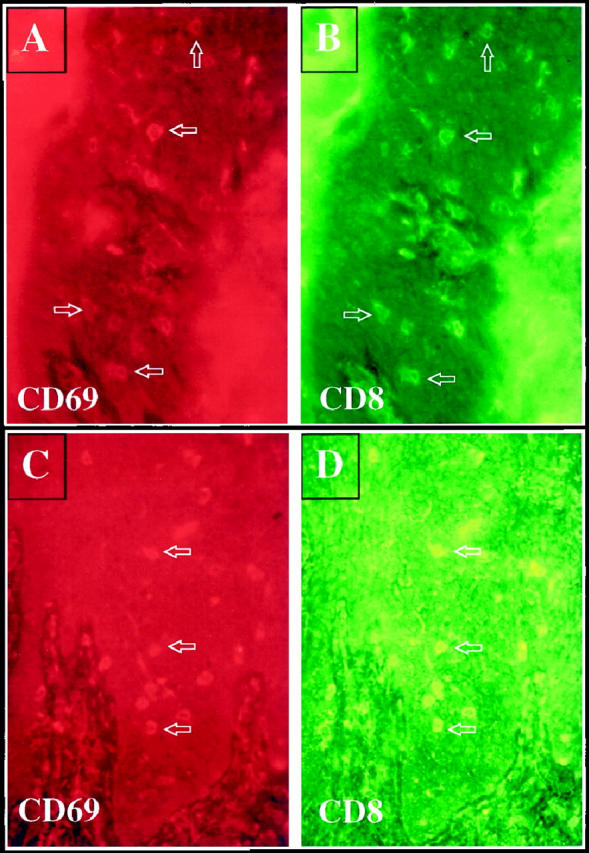
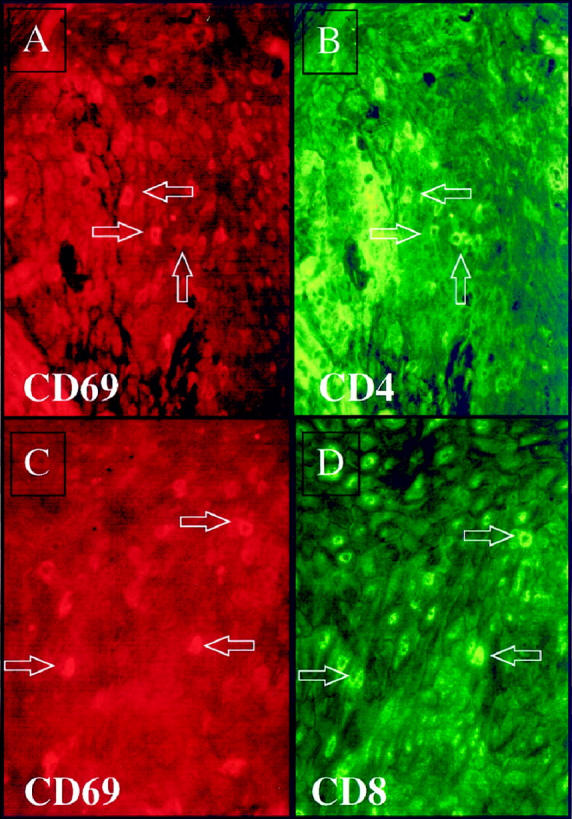
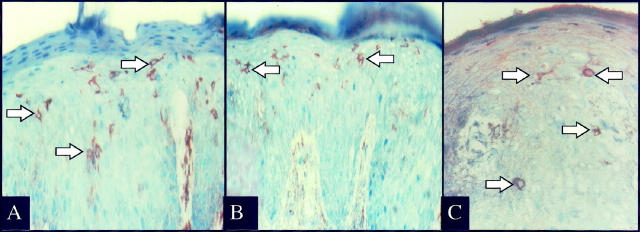
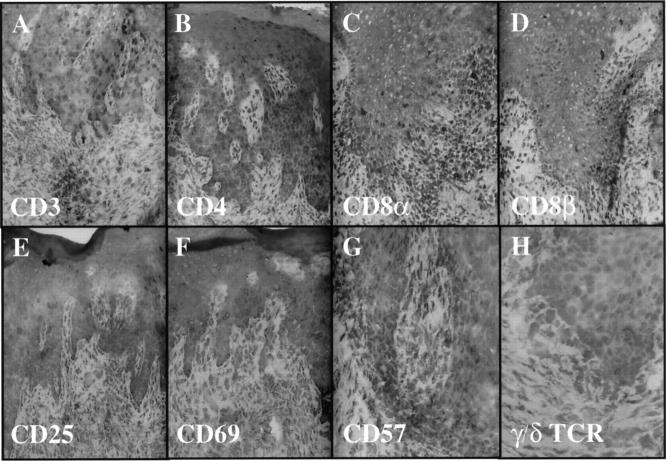
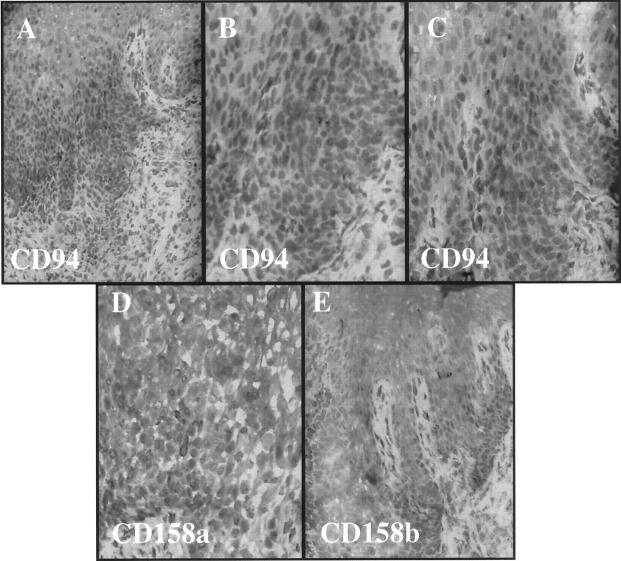
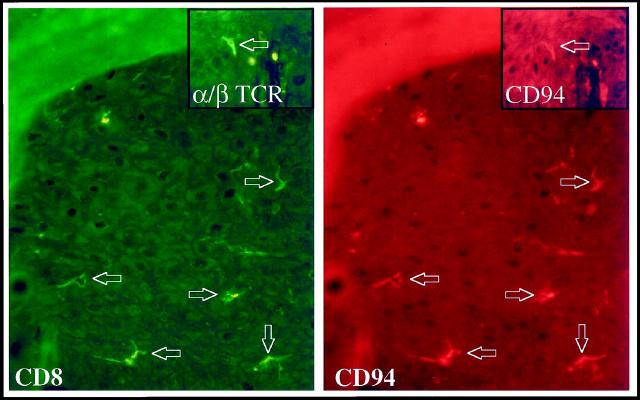
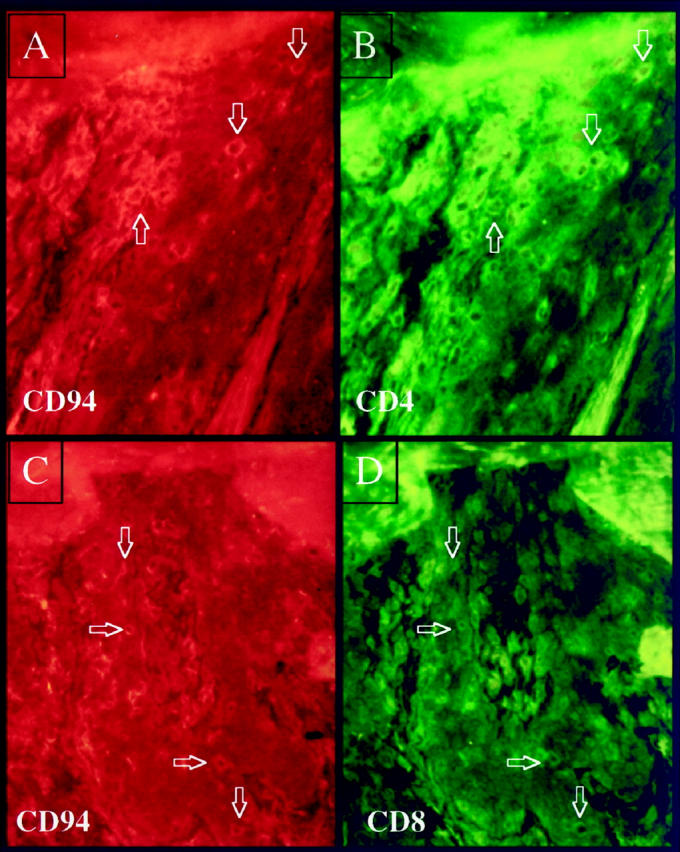
Psoriasis is an immunologically mediated skin disease linked to several different class I major histocompatibility complex alleles. However, the phenotype of the pathogenic lymphocyte and nature of the T cell activating event which triggers conversion of symptomless (PN) skin into psoriatic plaques (PP skin) is unknown. This study extends our previous observations in which autologous blood-derived immunocytes were injected into PN skin engrafted onto SCID mice to produce full-fledged PP lesions. The first question addressed is whether injected CD4+ T cells or CD8+ T cells were responsible for phenotypic conversion of PN to PP skin. In five different patients only CD4+ but not CD8+ T cell lines produced psoriatic lesions. Next, immunological events occurring within PN skin following injection of CD4+ T cells in grafts that had sufficient tissue available for detailed analysis was examined. In two patients, intraepidermal resident CD8+ T cells were induced to proliferate during lesion development, expressing acute activation markers CD25 and CD69. In another patient, injection of CD4+ T cells revealed CD69 expression by intraepidermal CD4+ as well as CD8+ T cells. To explore the molecular basis for local T cell activation and proliferation, we discovered that intraepidermal immunocytes, including both CD4 and CD8+ T cells, expressed surface receptors (ie, CD94, CD158a, CD158b) typically confined to natural killer cells (ie, natural killer receptors; NKRs) accumulated immediately before onset of acute lesions. The presence of NKR bearing immunocytes was also observed in 10 of 15 different biopsies of chronic plaques taken directly from patients, whereas PN skin (n = 8) or normal skin from healthy donors (n = 8), did not contain such NKR positive immunocytes. Of particular relevance to psoriasis is that these NKRs recognize various class I alleles including those typically inherited by psoriatic family members such as HLA-C and HLA-B allotypes. We conclude that injection of CD4+ T cells into PN skin triggers a series of local immunologically mediated stimulatory events that produce further T cell activation and appearance of both CD4 and CD8+ T cells that express NKRs.
Figures
References
-
- Farber EM, Reush MK, Glinski W, Karasek MA, Recht B, Nickoloff BJ: Perspectives on psoriasis. Farber EM Noll L Morhenn V Jacobs PH eds. Psoriasis: Proceedings of the Fourth International Symposium. 1987, :pp 3-9 Elsevier Press, New York
-
- Elder JT, Nair RP, Guo S, Henseler T, Christophers E, Voorhees JJ: The genetics of psoriasis. Arch Dermatol 1996, 127:881-884 - PubMed
-
- Takada S, Engleman E: Evidence for an association between CD8 molecules and the T cell receptor complex on apoptotic T cells. J Immunol 1987, 139:3231-3235 - PubMed
-
- Bos JD, Hulsebosch HJ, Krieg SR, Baxter PM, Cormane RM: Immunocompetent cells in psoriasis. Arch Dermatol Res 1983, 275:181-189 - PubMed
-
- Hanney H, Gu SQ, Johannesson A, Sundkrist KG, Biberfeld P: Subpopulations of mononuclear cells in microscopic lesions of psoriatic patients. Selective accumulation of suppressor/cytotoxic T cells in epidermis during the evolution of the lesion. J Invest Dermatol 1989, 83:416-420 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
