

Long-term follow-up of patients with rectal cancer managed by local excision with and without adjuvant irradiation
- PMID: 10400036
- PMCID: PMC1420844
- DOI: 10.1097/00000658-199907000-00008
Long-term follow-up of patients with rectal cancer managed by local excision with and without adjuvant irradiation
Abstract
Objective: The long-term outcomes of patients undergoing local excision with or without pelvic irradiation were examined to define the role of adjuvant irradiation after local excision of T1 and T2 rectal cancers.
Methods: Ninety-nine patients with T1 or T2 rectal cancers underwent local excision with or without adjuvant irradiation at Massachusetts General Hospital and Emory University Hospital between January 1966 and January 1997. Of these, 52 patients were treated by local excision alone and 47 patients by local excision plus adjuvant irradiation. Twenty-six of these 47 patients were treated by irradiation in combination with 5-fluorouracil chemotherapy. The outcomes of these groups were compared.
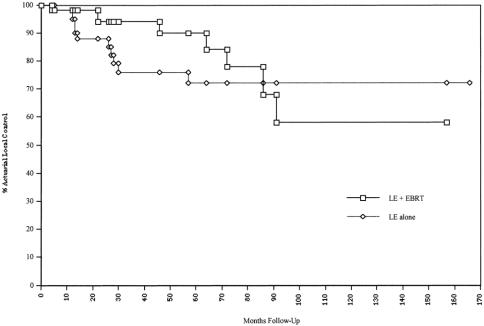
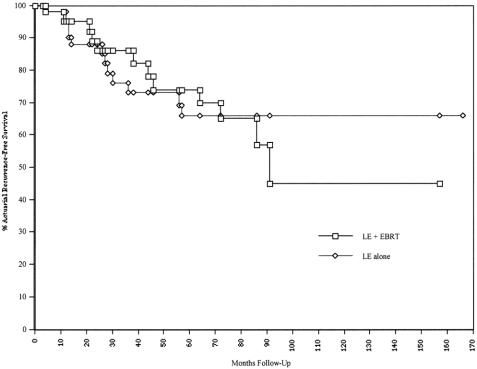
Results: The 5-year actuarial local control and recurrence-free survival rates were 72% and 66%, respectively, for the local excision alone group and 90% and 74%, respectively, for the adjuvant irradiation group. This improvement in outcome was evident despite the presence of a higher-risk patient population in the adjuvant irradiation group. Adverse pathologic features such as poorly differentiated histology and lymphatic or blood vessel invasion decreased local control and recurrence-free survival rates in the local excision only group. Adjuvant irradiation significantly improved 5-year outcomes in patients with high-risk pathologic features. Four cases of late local recurrence were seen at 64, 72, 86, and 91 months in the adjuvant irradiation group.
Conclusions: The authors recommend adjuvant chemoradiation for all patients undergoing local excision for T2 tumors, and for T1 tumors with high-risk pathologic features. The four cases of late local failures beyond 5 years in the adjuvant irradiation group underscores the need for careful long-term follow-up in these patients.
Figures
Comment in
-
Transanal endoscopic microsurgery (TEM).Ann Surg. 2000 Apr;231(4):614. doi: 10.1097/00000658-200004000-00025. Ann Surg. 2000. PMID: 10749624 Free PMC article. No abstract available.
References
-
- Wood WC, Willett CG. Update of the Massachusetts General Hospital experience of combined local excision and radiotherapy for rectal cancer. Surg Oncol Clin North Am 1992; 1: 131–136.
-
- Willett CG, Teppler JE, Donnelly S, et al. Patterns of failure following local excision and local excision and postoperative radiation therapy for invasive rectal adenocarcinoma. J Clin Oncol 1989; 8: 1003–1008. - PubMed
-
- Willett CG, Compton CC, Shellito PC, Efird JT. Selection factors for local excision or abdominoperineal resection of early stage rectal cancer. Cancer 1994; 73: 2716–2720. - PubMed
-
- Rosenthal SA, Yeung RS, Weese JL, et al. Conservative management of extensive low-lying rectal carcinomas with transanal local excision and combined preoperative and postoperative radiation therapy. A report of a phase I-II trial. Cancer 1992; 69: 335–341. - PubMed
-
- Minsky BD, Enker WE, Cohen AM, Lauwers G. Local excision and postoperative radiation therapy for rectal cancer. Am J Clin Oncol 1994; 17: 411–416. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
