

Clinical outcomes of acute myocarditis in childhood
- PMID: 10409542
- PMCID: PMC1729152
- DOI: 10.1136/hrt.82.2.226
Clinical outcomes of acute myocarditis in childhood
Abstract
Objective: To describe clinical outcomes of a paediatric population with histologically confirmed lymphocytic myocarditis.
Design: A retrospective review between November 1984 and February 1998.
Setting: A major paediatric tertiary care hospital.
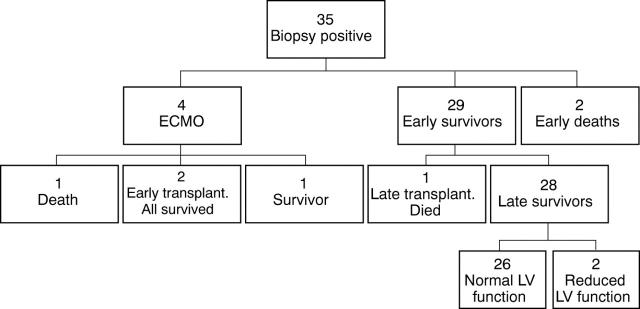
Patients: 36 patients with histologically confirmed lymphocytic myocarditis.
Main outcome measures: Survival, cardiac transplantation, recovery of ventricular function, and persistence of dysrhythmias.
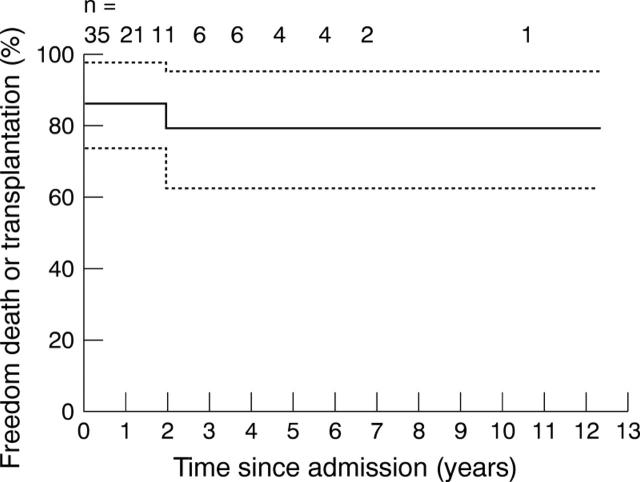
Results: Freedom from death or cardiac transplantation was 86% at one month and 79% after two years. Five deaths occurred within 72 hours of admission, and one late death at 1.9 years. Extracorporeal membrane oxygenation support was used in four patients, and three patients underwent heart replacement. 34 patients were treated with intravenous corticosteroids. In the survivor/non-cardiac transplantation group (n = 29), the median follow up was 19 months (range 1.2-131.6 months), and the median period for recovery of a left ventricular ejection fraction to > 55% was 2.8 months (range 0-28 months). The mean (SD) final left ventricular ejection and shortening fractions were 66 (9)% and 34 (8)%, respectively. Two patients had residual ventricular dysfunction. No patient required antiarrhythmic treatment. All survivors reported no cardiac symptoms or restrictions in physical activity.
Conclusions: Our experience documents good outcomes in paediatric patients presenting with acute heart failure secondary to acute lymphocytic myocarditis treated with immunosuppression. Excellent survival and recovery of ventricular function, with the absence of significant arrhythmias, continued cardiac medications, or restrictions in physical activity were the normal outcomes.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources