

Delays in protease inhibitor use in clinical practice
- PMID: 10417596
- PMCID: PMC1496613
- DOI: 10.1046/j.1525-1497.1999.08198.x
Delays in protease inhibitor use in clinical practice
Abstract
Objective: To determine the clinical factors associated with delayed protease inhibitor initiation.
Design: Chart review and telephone survey.
Setting: General medicine practice at an academic medical center in Boston, Mass.
Patients: One hundred ninety patients living with HIV and a viral load of more than 10,000 copies/ml.
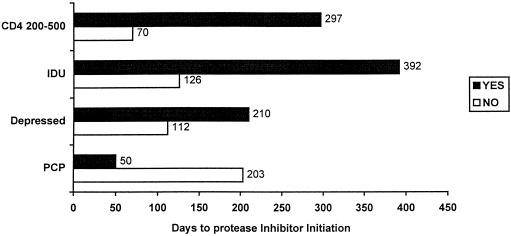
Measurements and main results: The main outcome measurement was time to first protease inhibitor prescription after first elevated HIV viral load (>10,000 copies/ml). In this cohort, 190 patients had an elevated viral load (median age 39; 87% male; 12% history of injection drug use; 63% AIDS; 53% with depression; 17% history of pneumocystis pneumonia; 54% CD4 <200). In Cox proportional hazards modeling, significant univariate correlates for delayed protease inhibitor initiation were higher CD4 cell count (hazard ratio [HR] 2. 38 for CD4 200-500 compared with <200, 95% confidence interval [CI] 1.59, 3.57; and HR 8.33 for CD4> 500; 95% CI 2.63, 25.0), higher viral load (HR 0.43 for each 10-fold increase; 95% CI 0.31, 0.59), injection drug use (HR 2.08; 95% CI 1.05, 4.17), AIDS (HR 0.24; 95% CI 0.15, 0.36), and history of pneumocystis pneumonia (HR 0.32; 95% CI 0.21, 0.49). In multivariate models adjusted for secular trends in protease inhibitor use, factors significantly associated with delay of protease inhibitor initiation (p <.05) were higher CD4 cell count (for CD4 200-500, HR 2.63; 95% CI 1.61, 4.17; for CD4> 500, HR 11.11; 95% CI 3.57, 33.33), higher viral load (HR 0.66 for each 10-fold increase; 95% CI 0.45, 0.98), history of pneumocystis pneumonia (HR 0.57; 95% CI 0.37, 0.90), history of depression (HR 1. 49; 95% CI 1.03, 2.13), and history of injection drug use (HR 2.70; 95% CI 1.35, 5.56).
Conclusions: HIV-infected patients with higher CD4 cell counts or a history of depression or history of injection drug use have significant and lengthy delays of protease inhibitor therapy. Although some delays may be clinically appropriate, enhancement of provider and patient education might prove beneficial. Further research should examine reasons for delays in protease inhibitor initiation and their appropriateness.
Figures
Comment in
-
When should we delay highly active antiretroviral therapy?J Gen Intern Med. 1999 Jul;14(7):446-8. doi: 10.1046/j.1525-1497.1999.05109.x. J Gen Intern Med. 1999. PMID: 10417605 Free PMC article. No abstract available.
References
-
- O'brien TR, Blattner WA, Waters D, et al. Serum HIV-1 RNA levels and time to development of AIDS in the Multicenter Hemophilia Cohort Study. JAMA. 1996;276:105–10. - PubMed
-
- Mellors JW, Kingsley LA, Rinaldo CR, et al. Quantitation of HIV-1 RNA in plasma predicts outcome after seroconversion. Ann Intern Med. 1995;122:573–9. - PubMed
-
- Perelson AS, Neumann AU, Markowitz M, Leonard JM, Ho DD. HIV-1 dynamics in vivo: virion clearance rate, infected cell life-span, and viral generation time. Science. 1996;271:1582–6. - PubMed
-
- Carpenter CCJ, Fischl MA, Hammer SM, et al. for the International AIDS Society. Antiretroviral Therapy for HIV infection in 1996: recommendations of an international panel. JAMA. 1996;276:146–54. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials