

Cardiac complications in children with human immunodeficiency virus infection. Pediatric Pulmonary and Cardiac Complications of Vertically Transmitted HIV Infection (P2C2 HIV) Study Group, National Heart, Lung, and Blood Institute
- PMID: 10429132
- PMCID: PMC4358844
- DOI: 10.1542/peds.104.2.e14
Cardiac complications in children with human immunodeficiency virus infection. Pediatric Pulmonary and Cardiac Complications of Vertically Transmitted HIV Infection (P2C2 HIV) Study Group, National Heart, Lung, and Blood Institute
Abstract
Objective: Although numerous cardiac abnormalities have been reported in HIV-infected children, precise estimates of the incidence of cardiac disease in these children are not well-known. The objective of this report is to describe the 2-year cumulative incidence of cardiac abnormalities in HIV-infected children.
Design: Prospective cohort (Group I) and inception cohort (Group II) study design.
Setting: A volunteer sample from 10 university and public hospitals.
Participants: Group I consisted of 205 HIV vertically infected children enrolled at a median age of 22 months. This group was comprised of infants and children already known to be HIV-infected at the time of enrollment in the study. Most of the children were African-American or Hispanic and 89% had symptomatic HIV infection at enrollment. The second group included 611 neonates born to HIV-infected mothers, enrolled during fetal life or before 28 days of age (Group II). In contrast to the older Group I children, all the Group II children were enrolled before their HIV status was ascertained.
Interventions: According to the study protocol, children underwent a series of cardiac evaluations including two-dimensional echocardiogram and Doppler studies of cardiac function every 4 to 6 months. They also had a 12- or 15-lead surface electrocardiogram (ECG), 24-hour ambulatory ECG monitoring, and a chest radiograph every 12 months.
Outcome measures: Main outcome measures were the cumulative incidence of an initial episode of left ventricular (LV) dysfunction, cardiac enlargement, and congestive heart failure (CHF). Because cardiac abnormalities tended to cluster in the same patients, we also determined the number of children who had cardiac impairment which we defined as having either left ventricular fractional shortening (LV FS) </=25% after 6 months of age, CHF, or treatment with cardiac medications.
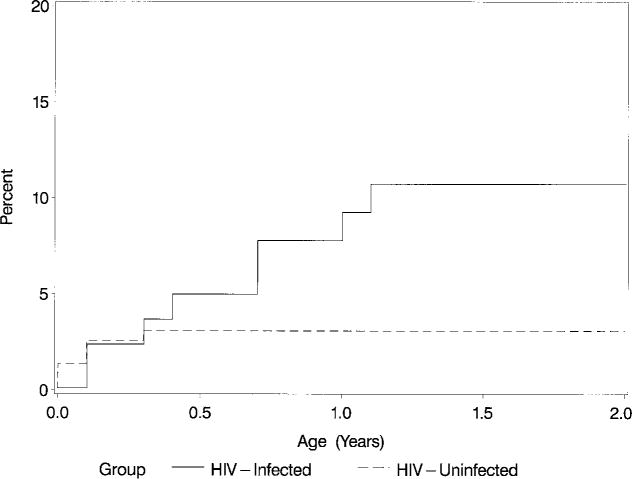
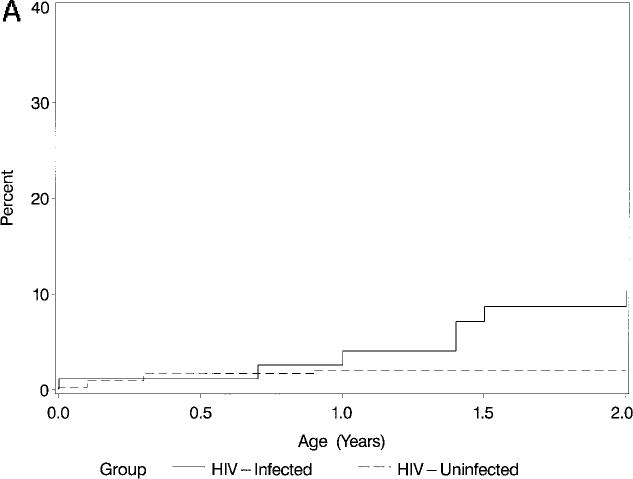
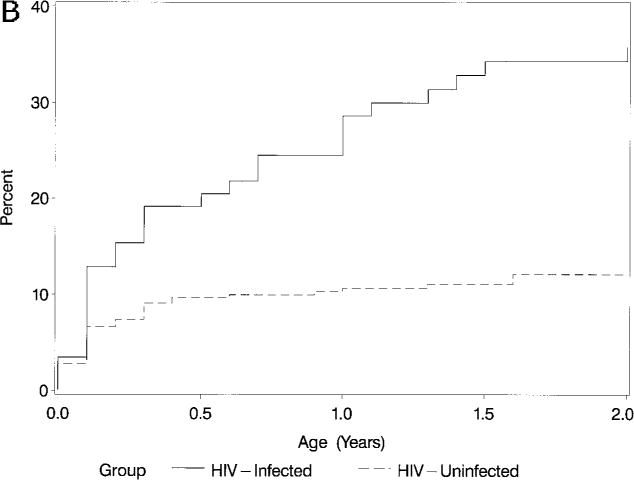
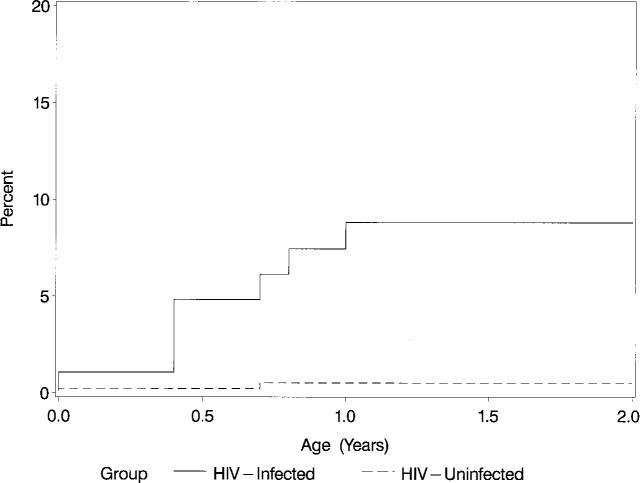
Results: CARDIAC ABNORMALITIES: In Group I children (older cohort), the prevalence of decreased LV function (FS </=25%) was 5.7% and the 2-year cumulative incidence (excluding prevalent cases) was 15.3%. The prevalence of echocardiographic LV enlargement (LV end-diastolic dimension z score >2) at the time of the first echocardiogram was 8. 3%. The cumulative incidence of LV end-diastolic enlargement was 11. 7% after 2 years. The cumulative incidence of CHF and/or the use of cardiac medications was 10.0% in Group I children. There were 14 prevalent cases of cardiac impairment (LV FS </=25% after 6 months of age, CHF, or treatment with cardiac medications) in Group I. After excluding these prevalent cases, the 2-year cumulative incidence of cardiac impairment was 19.1% among Group I children and 80.9% remained free of cardiac impairment after 2 years of follow-up. Within Group II (neonatal cohort), the 2-year cumulative incidence of decreased LV FS was 10.7% in the HIV-infected children compared with 3.1% in the HIV-uninfected children. LV dilatation was also more common in Group II infected versus uninfected children (8.7% vs 2.1%). The cumulative incidence of CHF and/or the use of cardiac medications was 8.8% in Group II infected versus 0.5% in uninfected subjects. The 1- and 2-year cumulative incidence rates of cardiac impairment for Group II infected children were 10.1% and 12.8%, respectively, with 87.2% free of cardiac impairment after the first 2 years of life.
Mortality: In the Group I cohort, the 2-year cumulative death rate from all causes was 16.9% [95% CI: 11.7%-22. 1%]. The 1- and 2-year mortality rates after the diagnosis of CHF (Kaplan-Meier estimates) were 69% and 100%, respectively. In the Group II cohort, the 2-year cumulative death rate from all causes was 16.3% [95% CI: 8.8%-23.9%] in the HIV-infected children compared with no deaths among the 463 uninfected Group II children. Two of the 4 Group II children with CHF died during the 2-year observation period and 1 more died within 2 years of the diagnosis of CHF. The 2-year mortality rate after the
Figures
References
-
- Lipshultz SE, Chanock S, Sanders SP, Colan SD, Perez-Atayde A, McIntosh K. Cardiac manifestations of human immunodeficiency virus infection in infants and children. Am J Cardiol. 1989;63:1489–1497. - PubMed
-
- Luginbuhl LM, Orav EJ, McIntosh K, Lipshultz SE. Cardiac morbidity and related mortality in children with HIV infection. JAMA. 1993;269:2869–2875. - PubMed
-
- Kovacs A, Hinton DR, Wright D, et al. Human immunodeficiency virus type 1 infection of the heart in three infants with acquired immunodeficiency syndrome and sudden death. Pediatr Infect Dis J. 1996;15:819–824. - PubMed
-
- Steinherz LJ, Brochstein JA, Robins J. Cardiac involvement in congenital acquired immunodeficiency syndrome. Am J Dis Child. 1986;140:1241–1244. - PubMed
-
- Stewart JM, Kaul A, Gromisch DS, Reyes E, Woolf PK, Gewitz MH. Symptomatic cardiac dysfunction in children with human immunodeficiency virus infection. Am Heart J. 1989;117:140–144. - PubMed
