

Three-dimensional reconstruction of pulmonary arteries in plexiform pulmonary hypertension using cell-specific markers. Evidence for a dynamic and heterogeneous process of pulmonary endothelial cell growth
- PMID: 10433934
- PMCID: PMC1866857
- DOI: 10.1016/S0002-9440(10)65137-1
Three-dimensional reconstruction of pulmonary arteries in plexiform pulmonary hypertension using cell-specific markers. Evidence for a dynamic and heterogeneous process of pulmonary endothelial cell growth
Abstract
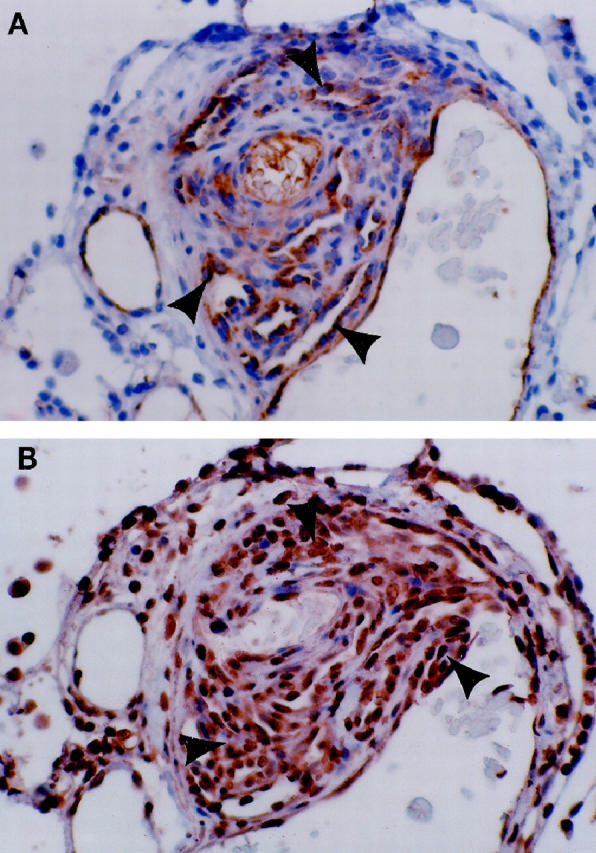
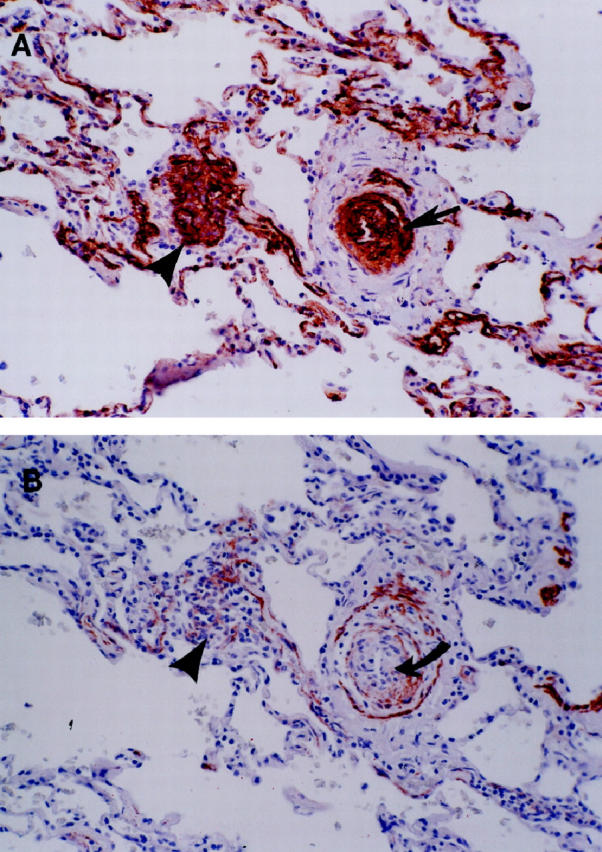
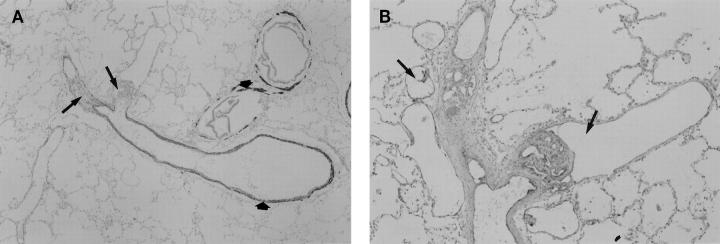
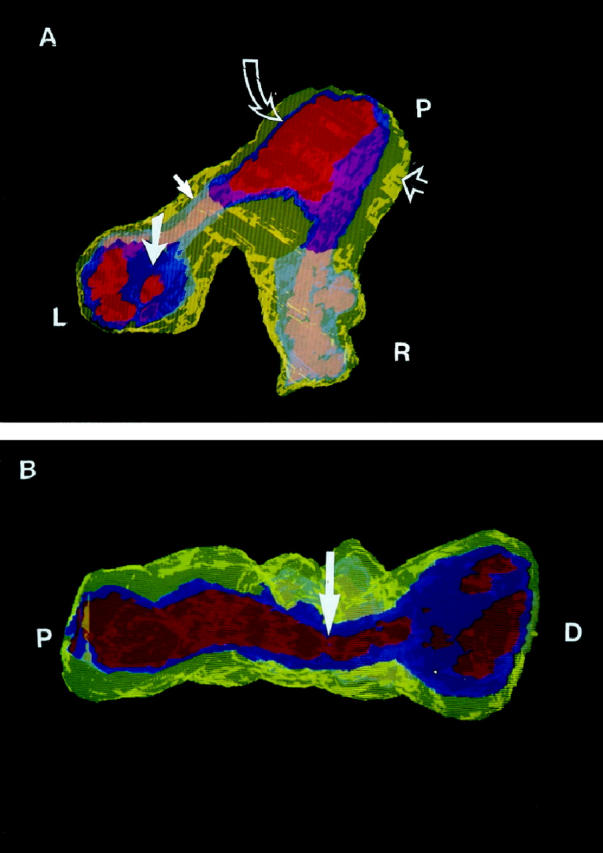
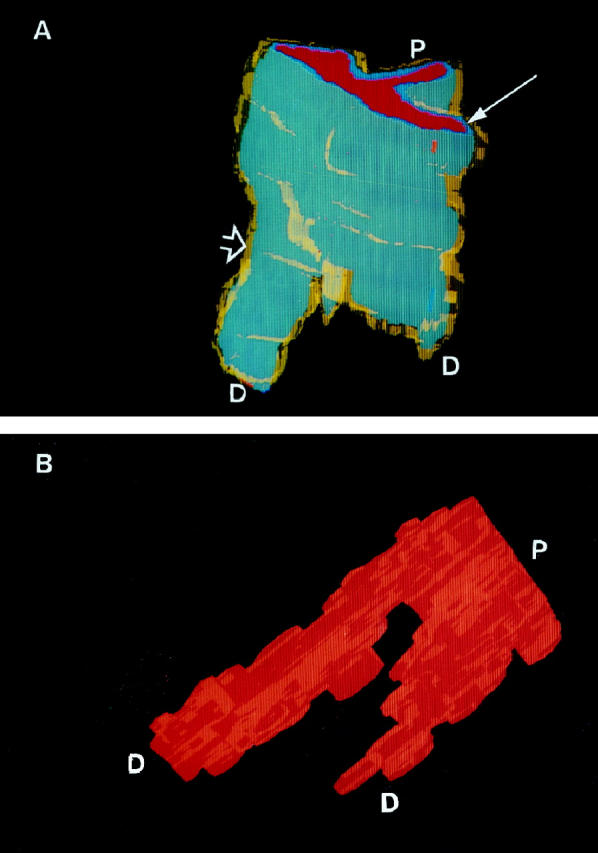
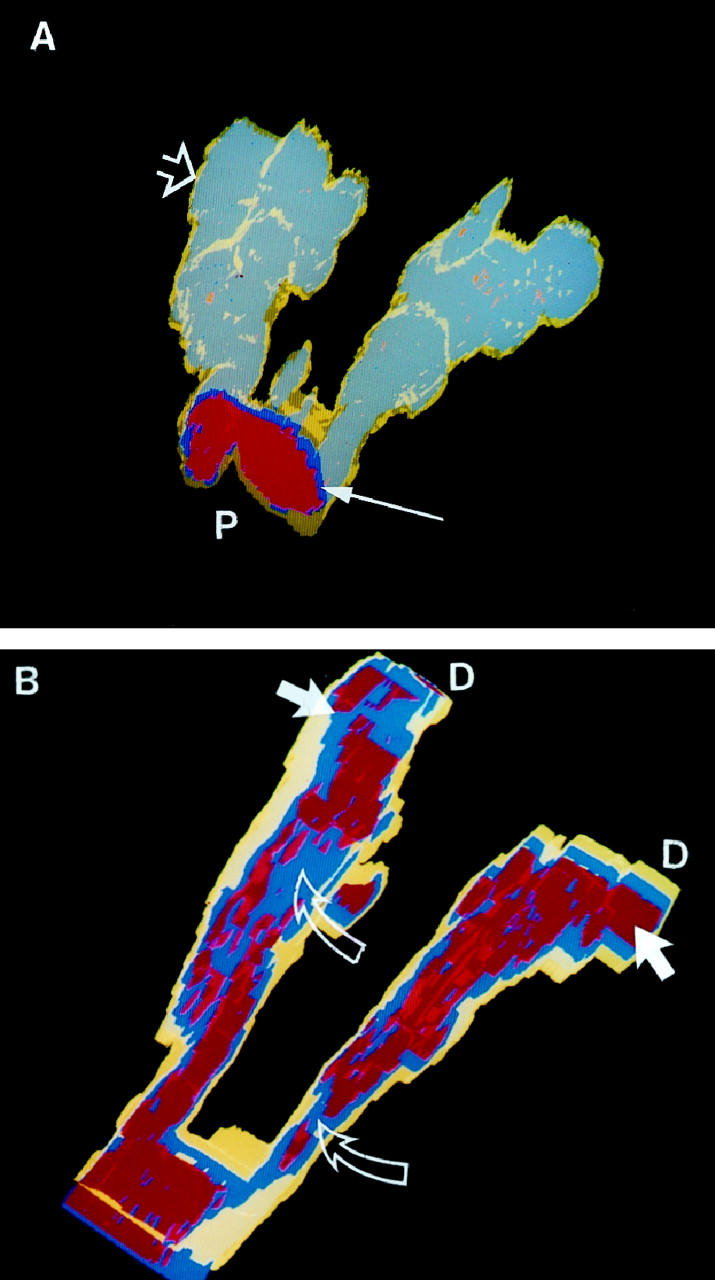
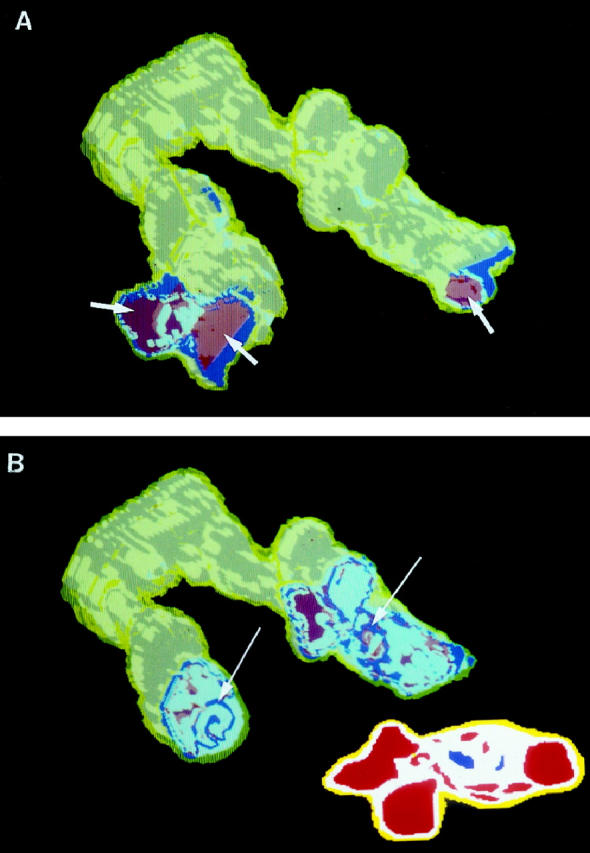
The plexiform lesions of severe pulmonary hypertension (PH) are complex vascular structures composed primarily of endothelial cells. In this study, we use immunohistochemical markers to identify the various cell layers of pulmonary vessels and to identify different endothelial cell phenotypes in pulmonary arteries affected by severe PH. Our computerized three-dimensional reconstructions of nine vessels in five patients with severe PH demonstrate that plexiform (n = 14) and concentric-obliterative (n = 6) lesions occur distal to branch points of small pulmonary arteries. And, whereas plexiform lesions occur as solitary lesions, concentric-obliterative lesions appear to be only associated with, and proximal to, plexiform structures. The endothelial cells of plexiform lesions express intensely and uniformly the vascular endothelial growth factor (VEGF) receptor KDR and segregate phenotypically into cyclin-kinase inhibitor p27/kip1-negative cells in the central core of the plexiform lesion and p27/kip1-positive cells in peripheral areas adjacent to incipient blood vessel formation. Using immunohistochemistry and three-dimensional reconstruction techniques, we show that plexiform lesions are dynamic vascular structures characterized by at least two endothelial cell phenotypes. Plexiform arteriopathy is not merely an end stage or postthrombotic change--it may represent one stage in an ongoing, angiogenic endothelial cell growth process.
Figures
Comment in
-
Plexiform lesion in severe pulmonary hypertension: association with glomeruloid lesion.Am J Pathol. 2001 Jul;159(1):382-3. doi: 10.1016/S0002-9440(10)61705-1. Am J Pathol. 2001. PMID: 11438486 Free PMC article. No abstract available.
References
-
- Wagenvoort CA, Wagenvoort N: Primary pulmonary hypertension. A histopathologic study of the lung vessels in 156 clinically diagnosed cases. Circulation 1970, 42:1163-1184
-
- Edwards, WD: Pathology of pulmonary hypertension. Cardiovasc Clin 1987, 18:321–354 - PubMed
-
- Robalino BD, Moodie DS: Association between primary pulmonary hypertension and portal hypertension: analysis of its pathophysiology and clinical, laboratory and hemodynamic manifestations. J Am Coll Cardiol 1991, 17:492-498 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
