

Primary cutaneous CD8-positive epidermotropic cytotoxic T cell lymphomas. A distinct clinicopathological entity with an aggressive clinical behavior
- PMID: 10433941
- PMCID: PMC1866866
- DOI: 10.1016/S0002-9440(10)65144-9
Primary cutaneous CD8-positive epidermotropic cytotoxic T cell lymphomas. A distinct clinicopathological entity with an aggressive clinical behavior
Abstract
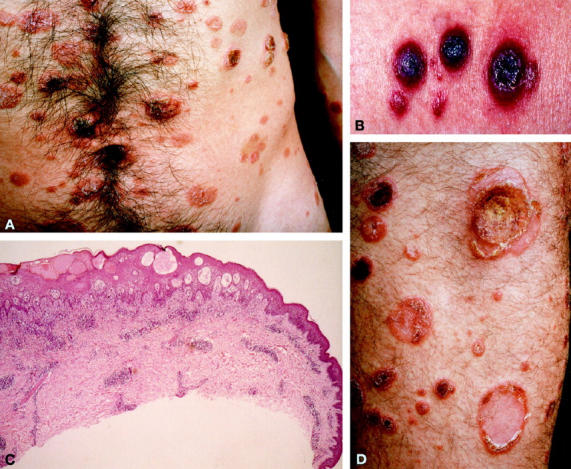
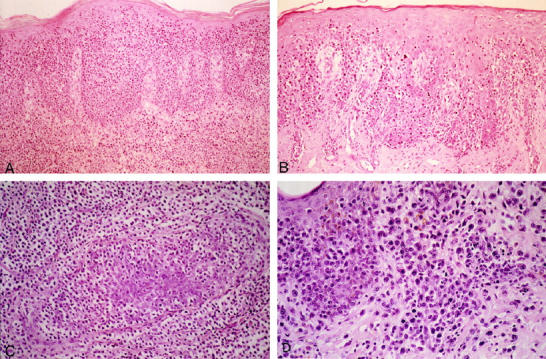
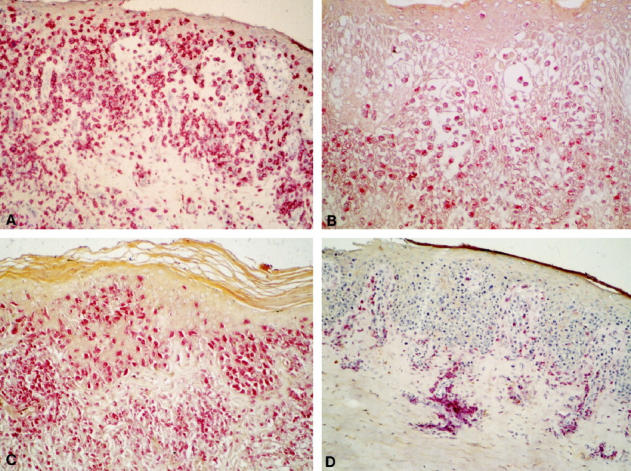
Cutaneous T cell lymphomas (CTCL) generally have the phenotype of CD3+, CD4+, CD45RO+ memory T cells. CTCL expressing a CD8+ T cell phenotype are extremely rare and ill-defined. To elucidate whether these CD8+ CTCL represent a distinct disease entity, the clinical, histological, and immunophenotypical features of 17 CD8+ CTCL were reviewed. None of the 17 cases expressed markers characteristic of natural killer cells or gamma/delta T cells. Nine of 17 cases showed the characteristic clinical and histological features as well as clinical behavior of well defined types of CTCL, such as mycosis fungoides (2 cases), pagetoid reticulosis (2 cases), lymphomatoid papulosis (2 cases), and CD30+ large T cell lymphoma (2 cases), all of which usually express a CD4+ T cell phenotype, and 1 case of subcutaneous panniculitis-like T cell lymphoma. The other 8 cases formed a homogeneous group showing a distinctive set of clinicopathological and immunophenotypical features, not consistent with that of other well defined types of CTCL. Clinical characteristics included presentation with generalized patches, plaques, papulonodules, and tumors mimicking disseminated pagetoid reticulosis; metastatic spread to unusual sites, such as the lung, testis, central nervous system, and oral cavity, but not to the lymph nodes; and an aggressive course (median survival, 32 months). Histologically, these lymphomas were characterized by band-like infiltrates consisting of pleomorphic T cells or immunoblasts, showing a diffuse infiltration of an acanthotic epidermis with variable degrees of spongiosis, intraepidermal blistering, and necrosis. The neoplastic cells showed a high Ki-67 proliferation index and expression of CD3, CD8, CD7, CD45RA, betaF1, and TIA-1 markers, whereas CD2 and CD5 were frequently lost. Expression of TIA-1 pointed out that these lymphomas are derived from a cytotoxic T cell subset. The results of this and other studies reviewed herein suggest that these strongly epidermotropic primary cutaneous CD8+ cytotoxic T cell lymphomas represent a distinct type of CTCL with an aggressive clinical behavior.
Figures
References
-
- Willemze R, Kerl H, Sterry W, Berti E, Cerroni L, Chimenti S, Diaz-Perez JL, Geerts ML, Goos M, Knobler R, Ralfkiaer E, Santucci M, Smith N, Wechsler J, van Vloten WA, Meijer CJ: EORTC classification for primary cutaneous lymphomas: a proposal from the cutaneous lymphoma study group of the european organization for research and treatment of cancer. Blood 1997, 90:354-371 - PubMed
-
- Caputo R, Berti E, Monti M, Cavicchini S: A verrucoid epidermotropic OKT8-positive lymphoma. Am J Dermatopathol 1983, 5:159-164 - PubMed
-
- Buechner SA, Winkelmann RK, Banks PM: T cells and T-cell subsets in mycosis fungoides and parapsoriasis. A study of 18 cases with anti-human T cell monoclonal antibodies and histochemical techniques. Arch Dermatol 1984, 120:897–905 - PubMed
-
- Deneau DG, Wood GS, Beckstead J, Hoppe RT, Price N: Woringer-Kolopp disease (pagetoid reticulosis): four cases with histopathologic, ultrastructural, and immunohistologic observations. Arch Dermatol 1984, 120:1045-1051 - PubMed
-
- Mackie RM, Turbitt ML: A case of pagetoid reticulosis bearing the cytotoxic suppressor surface marker on the lymphoid infiltrate: further evidence that pagetoid reticulosis is not a variant of mycosis fungoides. Br J Dermatol 1984, 110:89-94 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
