

Allo-limbal transplantation in patients with limbal stem cell deficiency
- PMID: 10434862
- PMCID: PMC1722986
- DOI: 10.1136/bjo.83.4.414
Allo-limbal transplantation in patients with limbal stem cell deficiency
Abstract
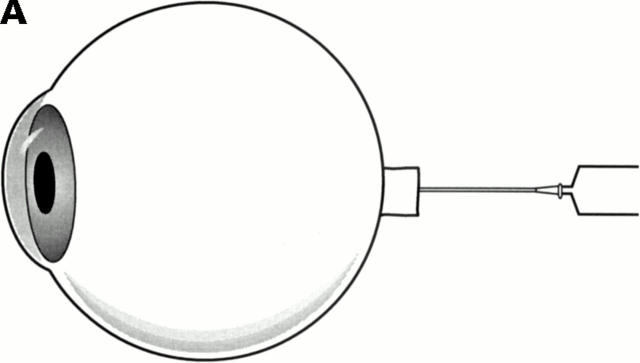
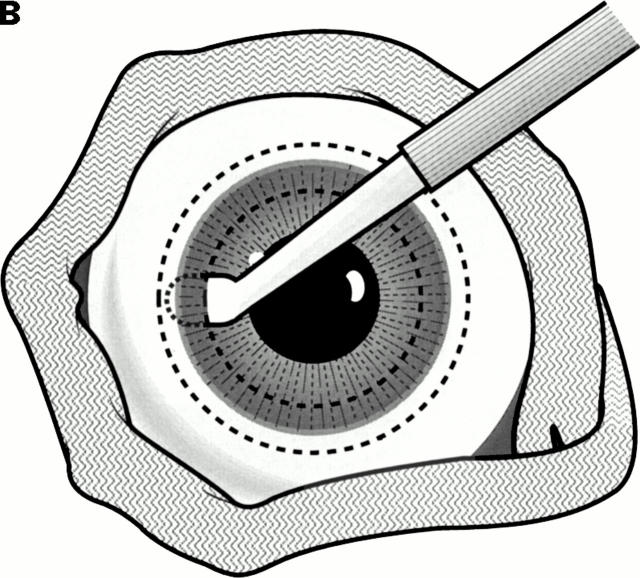
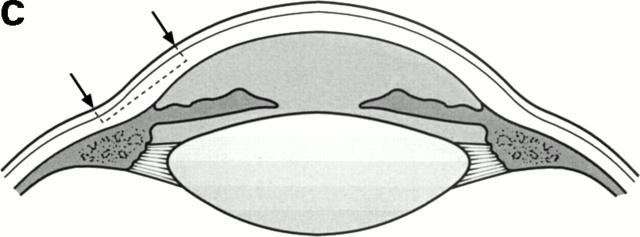
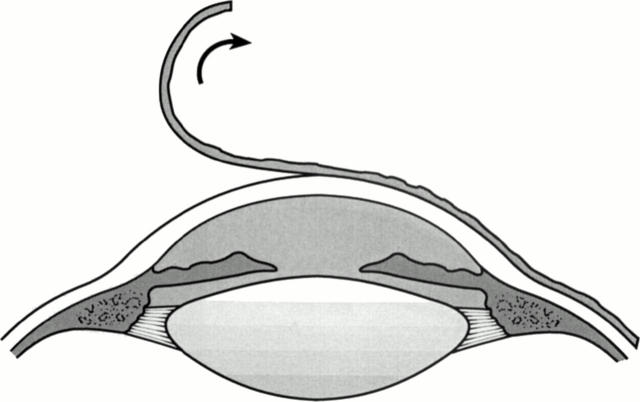
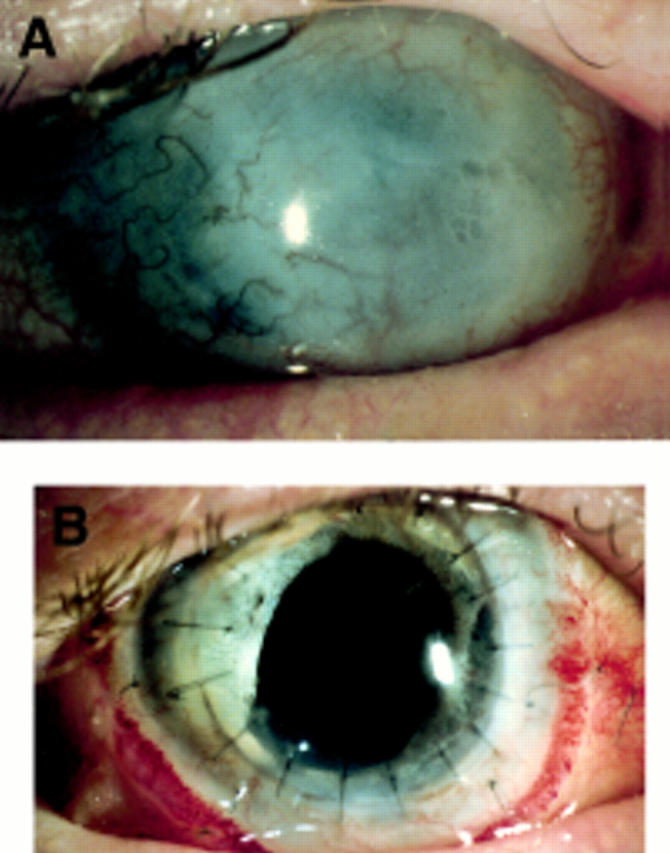
Aim: To report the outcome of a series of patients with stem cell deficiency who underwent allo-limbal transplantation and to describe a technique for this procedure.
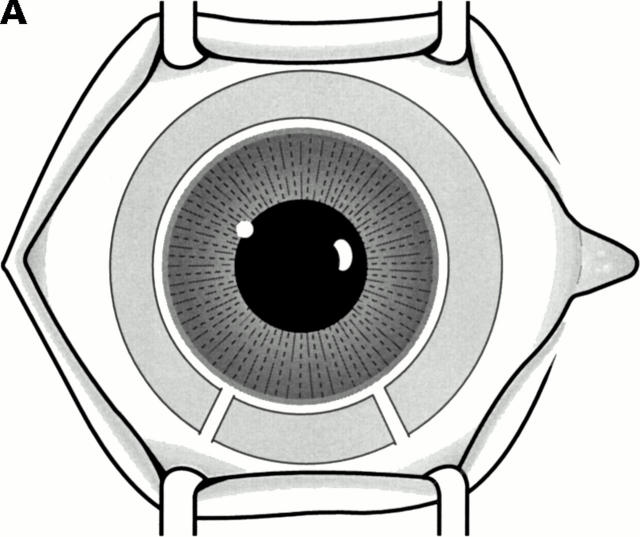
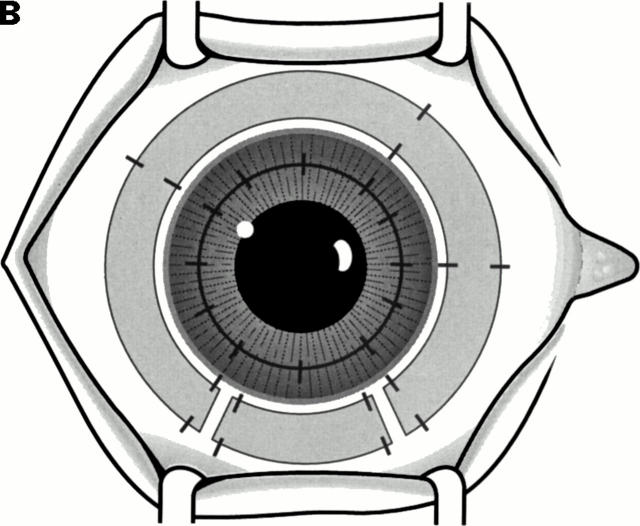
Methods: Six consecutive patients underwent allo-limbal stem cell transplantation. The primary diagnosis included alkali burn (n = 2), trachoma (n = 1), chronic rosacea blepharitis and kerato-conjunctivitis (n = 1), aniridia (n = 1), and Stevens-Johnson syndrome (n = 1). The limbal rim consisted of peripheral cornea and perilimbal sclera. FK-506 was used postoperatively for immunosuppression.
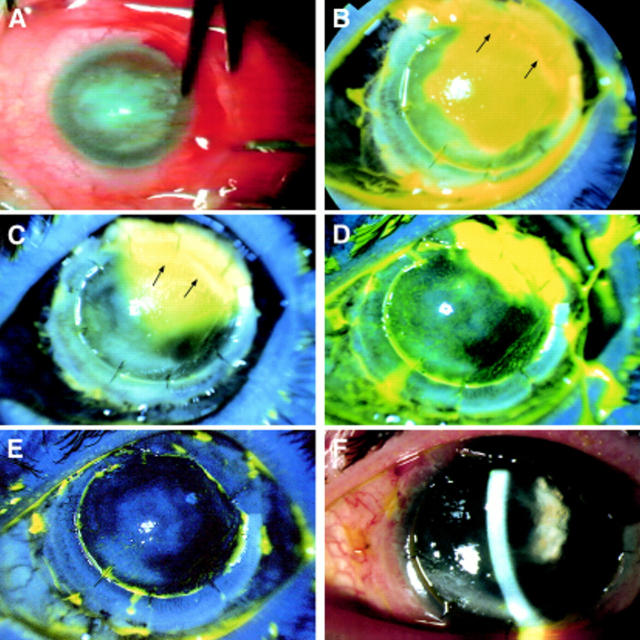
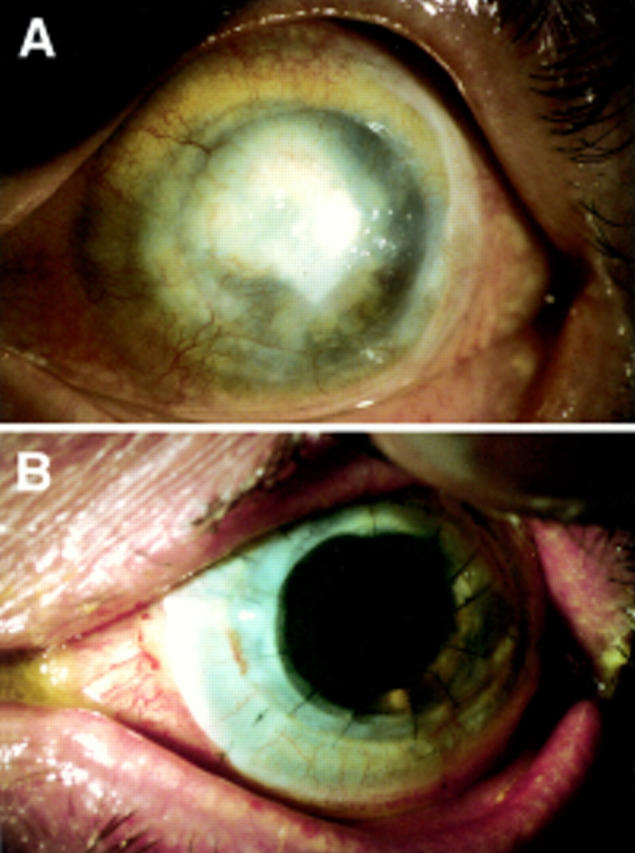
Results: The length of follow up ranged from 3 to 24 months (mean follow up 11.8 (SD 9.3) months). The outcome was considered satisfactory in five of six cases. The corneal surface was completely epithelialised within 2 weeks, and there was a substantial improvement in vision and symptoms. One patient had recurrent epithelial defects related to eyelid abnormalities. No side effects associated with systemic immunosuppression were noted.
Conclusion: Allo-limbal transplantation, with systemic immunosuppression with FK-506 is useful in reconstruction of the ocular surface with improvement in vision in patients with severe stem cell deficiency.
Figures
Comment in
-
Allo-limbal transplantation in patients with limbal stem cell deficiency.Br J Ophthalmol. 1999 Dec;83(12):1409. doi: 10.1136/bjo.83.12.1409. Br J Ophthalmol. 1999. PMID: 10574823 Free PMC article. No abstract available.
-
Limbal allografting using FK-506.Br J Ophthalmol. 1999 Dec;83(12):1409-10. doi: 10.1136/bjo.83.12.1409a. Br J Ophthalmol. 1999. PMID: 10574824 Free PMC article. No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical