

Endoscopic laser recanalisation of presaccal canalicular obstruction
- PMID: 10434867
- PMCID: PMC1723005
- DOI: 10.1136/bjo.83.4.443
Endoscopic laser recanalisation of presaccal canalicular obstruction
Abstract
Aim: To document the results of erbium (Er)-YAG laser treatment in presaccal canalicular obstruction in combination with the use of a flexible endoscope.
Methods: For the first time an Er-YAG laser (Schwind, Sklerostom) was attached to a flexible endoscope (Schwind, Endognost) and used to recanalise a stenosis of the upper, lower, or common canaliculus. In 17 patients (mean age 41.5 (SD 11.9) years), 19 treatments (two bilateral) were performed. In all cases the scar was observed using the endoscope and was excised by laser ablation. A silicone intubation was performed in all cases. In addition to the endoscopy an irrigation was performed to prove the intactness of the lacrimal pathway system after laser treatment.
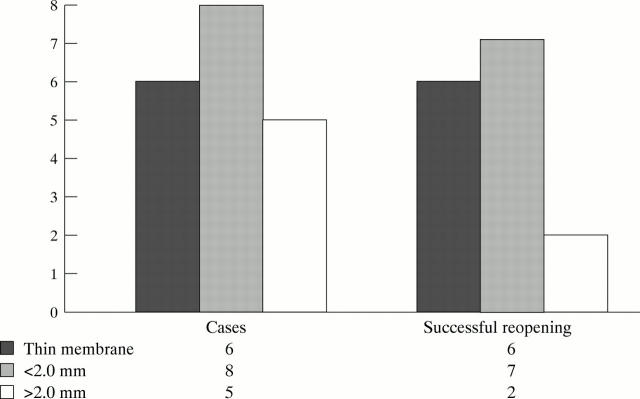
Results: Membranous obstructions with a maximum length of 2.0 mm (14 procedures) in the canaliculus were opened easily using the laser, and the silicone intubation was subsequently performed without difficulty. Scars thicker than 2.0 mm could not be opened safely without canaliculus penetration (five procedures). Irrigation was positive in all cases up to the end of a 6 month period, providing the tubes remained in place. The maximum follow up is now 17 months (minimum 8 months) and in 16 cases (84.2%) the canaliculi are still intact.
Conclusion: Endoscopic laser treatment combined with silicone intubation enables us to recanalise presaccal stenoses of canaliculi under local anaesthesia up to a scar thickness of 2.0 mm. Best results can be achieved in cases where much tissue can be saved. Under such conditions this procedure can substitute for more invasive surgical techniques, especially a conjunctivo-dacryocystorhinostomy (CDCR).
Figures





References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical