

Immunolocalisation of the VEGF receptors FLT-1, KDR, and FLT-4 in diabetic retinopathy
- PMID: 10434875
- PMCID: PMC1722996
- DOI: 10.1136/bjo.83.4.486
Immunolocalisation of the VEGF receptors FLT-1, KDR, and FLT-4 in diabetic retinopathy
Abstract
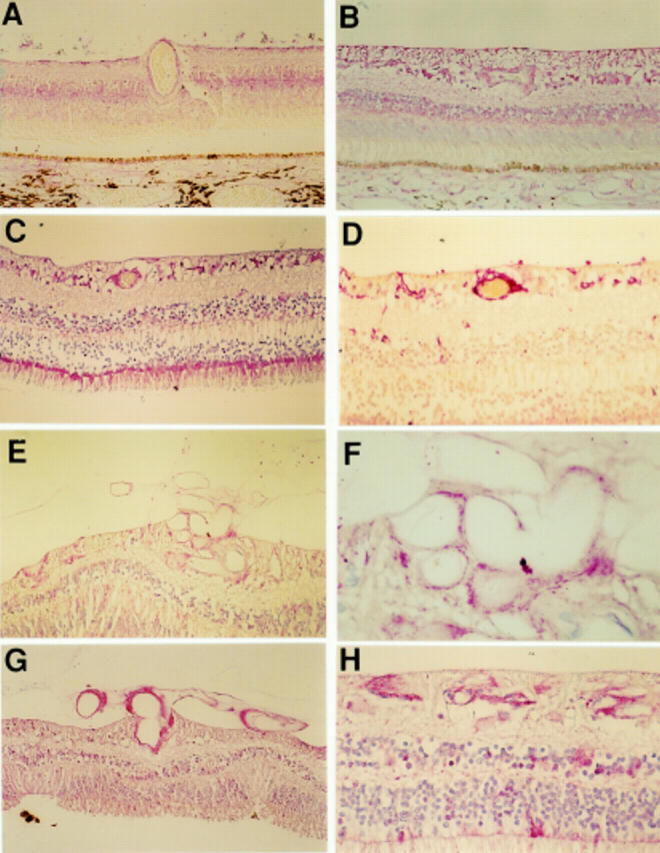
Aim: To determine the spatial and temporal changes in the staining pattern of the VEGF receptors FLT-1, KDR, and the putative receptor FLT-4 during the pathogenesis of diabetic retinopathy.
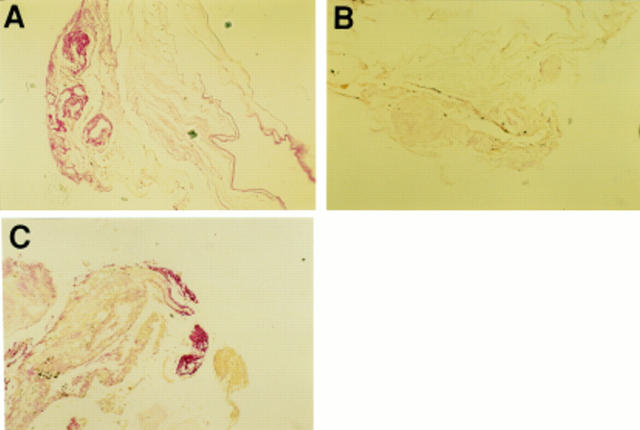
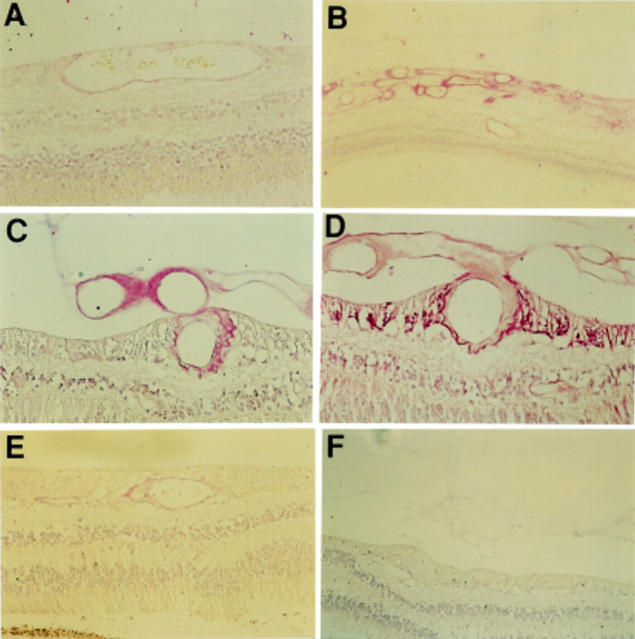
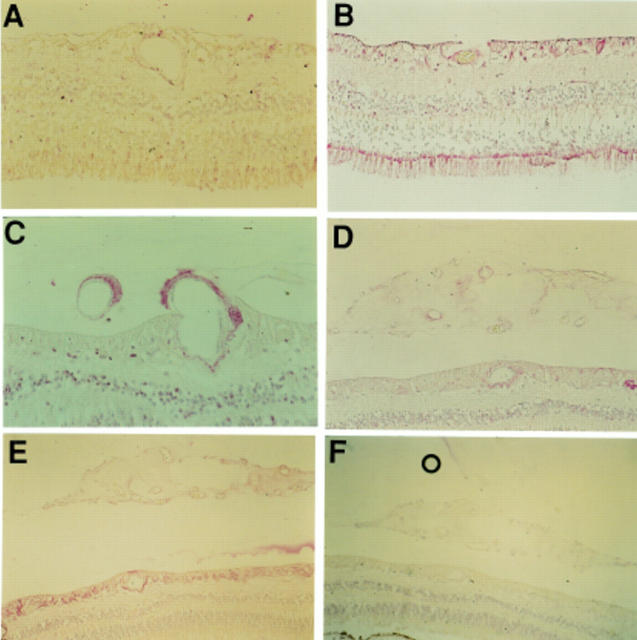
Methods: Immunohistochemical localisation of VEGF receptors, using antibodies against FLT-1, FLT-4, and KDR, was carried out on specimens of normal human retina (n = 10), diabetic retinas (a) with no overt retinopathy (n = 12), (b) with intraretinal vascular abnormalities but no proliferative retinopathy (n = 5), (c) with active proliferative retinopathy (n = 6), and (d) with no residual proliferative retinopathy after scatter photocoagulation therapy (n = 14), and surgically excised diabetic fibrovascular membranes (n = 11). The degree and pattern of immunostaining was recorded.
Results: FLT-1 staining was apparent in the retinas from both non-diabetic and diabetic retinas; weak to moderate staining was generally confined to the inner nuclear layer, the ganglion cell layer, and the retinal vessels during all stages of the disease process. Staining of the retinal vessels was raised in diabetic tissue compared with non-diabetic tissue. The preretinal vessels of the diabetic subjects stained moderately to intensely for FLT-1. In contrast with FLT-1 staining minimal immunostaining for KDR was demonstrated in the non-diabetic eyes and the unlasered eyes; however, weak staining for KDR was observed in the inner nuclear layer and the ganglion cell layer of the unlasered eyes with diabetic changes. In those retinas with preretinal neovascularisation KDR immunoreactivity was moderate to intense in the intra- and preretinal vessels. However, in the excised membranes, where the vessels may have been in a quiescent state, the levels of KDR were weak to moderate. After apparently successful laser treatment KDR staining was reduced in the intraretinal vessels. Minimal FLT-4 staining was observed throughout normal eyes while weak to moderate FLT-4 staining was generally confined to the inner nuclear layer and the ganglion cell layer of the unlasered diabetic eyes. Weak to moderate levels of FLT-4 staining were observed in the intraretinal vessels except after apparently successful laser treatment where reduced levels of staining were observed. Weak to moderate staining was observed in the preretinal vessels.
Conclusions: This study supports a role for FLT-1, KDR, and possibly FLT-4 in the pathogenesis of diabetic retinopathy; however, their specific roles in the progression of the disease may differ.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous