

CNS involvement in neuro-Behçet syndrome: an MR study
- PMID: 10445437
- PMCID: PMC7056254
CNS involvement in neuro-Behçet syndrome: an MR study
Abstract
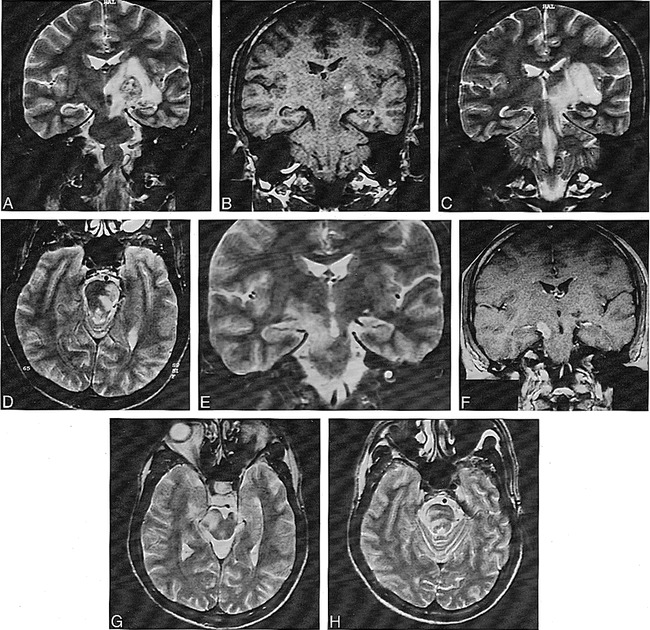
Background and purpose: Behçet disease (BD) is a multisystem vasculitis of unknown origin in which neurologic involvement has been reported in the range of 5% to 10% in large series. Reports on clinical and radiologic aspects of neuro-Behçet syndrome (NBS) are in general limited in number. Our purpose was to determine the MR patterns in patients with NBS who had neural parenchymal involvement and to correlate our findings with possible vascular pathophysiology.
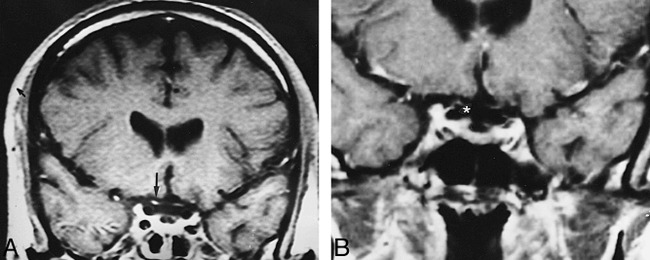
Methods: The MR images of 65 patients with NBS and neural parenchymal involvement were reviewed. In a subgroup of patients who had serial MR studies, we evaluated the anatomic-radiologic location and distribution of the lesions and whether they corresponded to any vascular territory, and studied their extension, enhancement patterns, and temporal course.
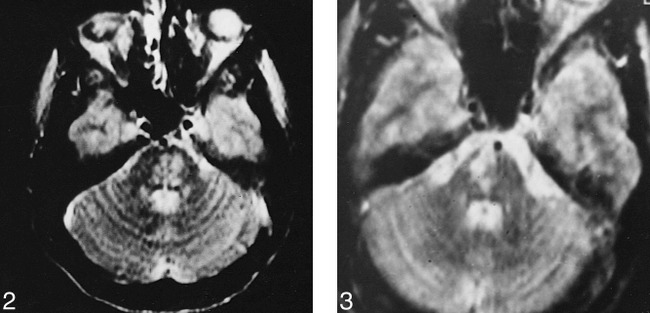
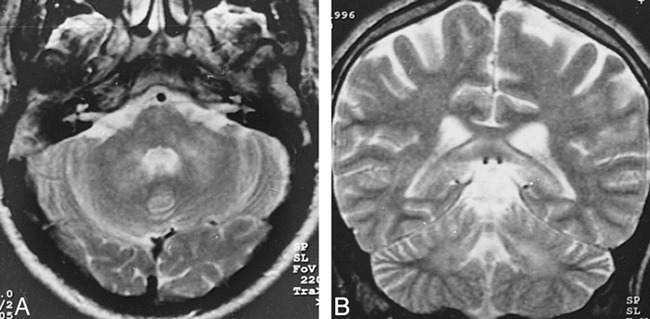
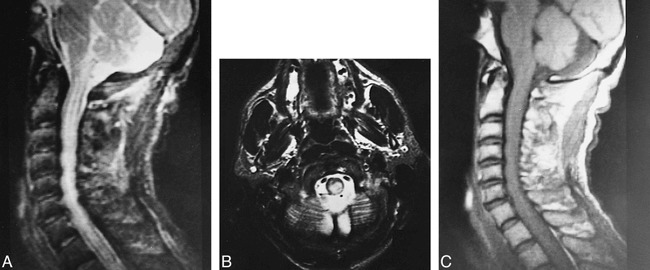
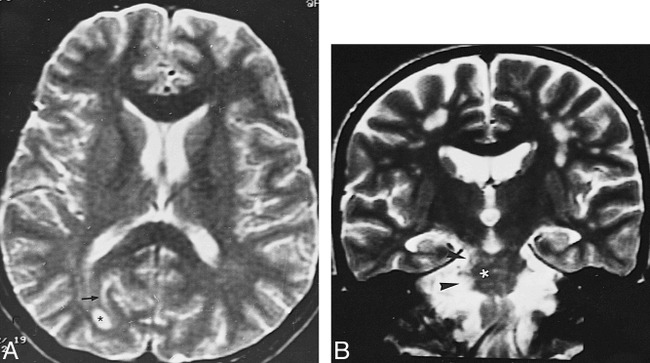
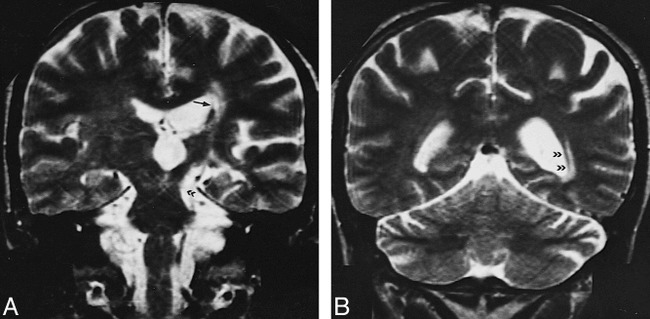
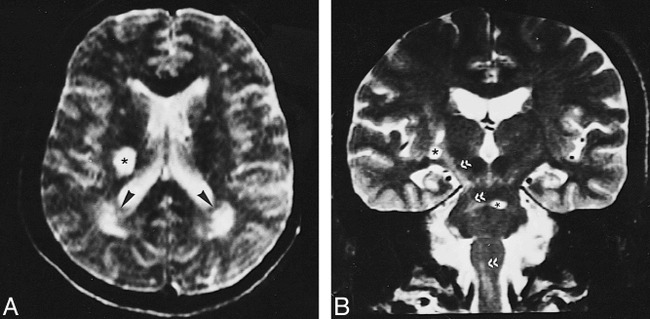
Results: The most common imaging finding in NBS patients who had neural parenchymal involvement was a mesodiencephalic junction lesion with edema extending along certain long tracts in the brain stem and diencephalon in 46% of the patients. The next most common location of involvement was the pontobulbar region, seen in 40% of the cases. Three primary cervical spinal cord lesions and one case of isolated optic nerve involvement were observed.
Conclusion: The parenchymal distribution of lesions in NBS appears to support the hypothesis of small-vessel vasculitis; mainly, venular involvement. The anatomic distribution of intraaxial veins of the CNS explains the predominant involvement of the brain stem structures observed in our patients. This pattern of lesion distribution might help to differentiate NBS from other vasculitides as well as from the inflammatory-demyelinating diseases of the CNS, such as multiple sclerosis.
Figures

References
-
- Behçet H. Uber residivierende, aphtöse, durch ein virus verursachte Geschwüre am Mund, am Auge und an den Genitalien. Derm Woschenscr 1937;105:1152-1157
-
- Yazici H, Yurdakul S, Hamuryudan V. Behçet's syndrome. In: Klippel J, Dieppe P, eds. Rheumatology. London: Gower Medical; 1997;7.26:1–6
-
- O'Duffy JD. Vasculitis in Behçet's disease. Rheum Dis Clin North Am 1990;16:423-431 - PubMed
-
- Lakhanpal S, Tani K, Lie JT, Katoh K, Ishigatsuba Y, Ohokubo T. Pathological features of Behçet's syndrome: a review of Japanese autopsy registry data. Hum Pathol 1985;16:790-795 - PubMed
-
- Inaba G. Clinical features of neuro-Behçet syndrome. In: Lehner T, Barnes CG, eds. Recent Advances in Behçet's Disease. International Congress and Symposium Series Number 103. London: Royal Society of Medicine Services; 1986:235–246
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous