

Recurrent carotid blowout syndrome: diagnostic and therapeutic challenges in a newly recognized subgroup of patients
- PMID: 10445446
- PMCID: PMC7056216
Recurrent carotid blowout syndrome: diagnostic and therapeutic challenges in a newly recognized subgroup of patients
Abstract
Background and purpose: To our knowledge, recurrent carotid blowout syndrome (rCBS) has not been well described. Our purpose was to review our institution's recent experience with patients who presented with multiple episodes of carotid blowout syndrome (CBS), and who were referred for emergent diagnostic angiography and endovascular therapy.
Methods: We retrospectively reviewed the last 46 consecutive patients who had a clinical diagnosis of CBS. All patients were examined and treated prospectively according to a standardized protocol. Most patients (43 of 46) had undergone extensive primary and salvage radical surgery with intraoperative brachytherapy or external beam radiation or both. The remaining three patients had either traumatic or iatrogenic CBS.
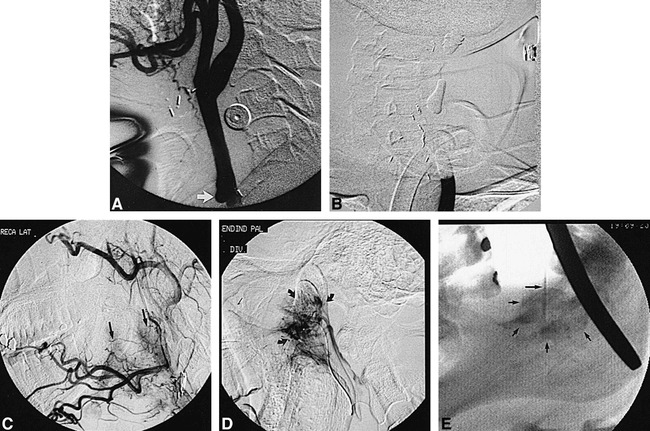
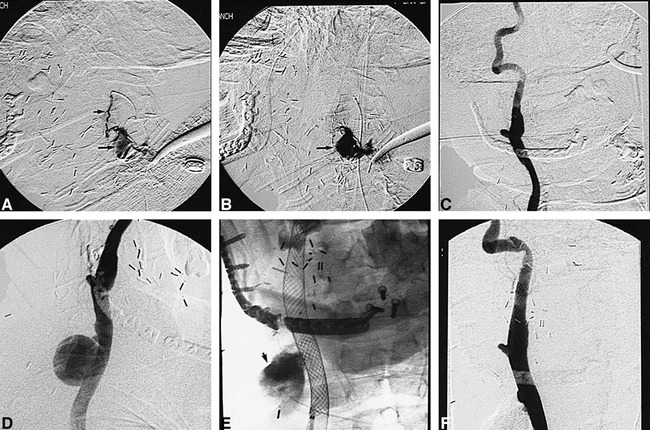
Results: Twelve patients (26%) in our series had more than one episode of CBS in which a total of 32 (20 recurrent) events were observed (average 2.7, range 2-4). Intervals of rCBS ranged from 1 day to 6 years. Thirteen (65%) of 20 recurrent events were attributed to progressive disease (PD), and seven (35%) of 20 to treatment failures (TFs). In the PD group, seven (54%) of 13 had recurrent ipsilateral disease, and six (46%) of 13 had recurrent contralateral disease. Etiologies of rCBS were as follows: seven exposed carotids; seven carotid pseudoaneurysms; eight small-branch pseudoaneurysms; five tumor hemorrhages; three hyperemic/ulcerated wounds; and one aortic arch rupture. Twenty-seven of 32 events were treated with endovascular therapy, which included the following: nine carotid occlusions; 11 small-branch embolizations; three transarterial tumor embolizations; one carotid stent; and two direct-puncture embolizations. Four of six TFs were retreated successfully with endovascular therapy; the remaining two TFs were managed successfully by surgery. In the PD group, hemorrhagic complications of rCBS were managed successfully in all but one patient, who died. No permanent neurologic or ophthalmologic complications occurred.
Conclusion: Recurrent CBS is a frequently encountered problem in which most cases are caused by PD resulting from both multifocal iatrogenic arteriopathy and occasional wound complications that are characteristic of aggressively managed head and neck surgical patients. Initial TFs are encountered often as well. Despite the diagnostic and therapeutic challenges of rCBS, most cases can be retreated effectively.
Figures
References
-
- Citardi MJ, Chaloupka JC, Son YH, Sasaki CT. Management of carotid artery rupture by monitored endovascular therapeutic occlusion (1988–1994). Laryngoscope 1995;1086-1092 - PubMed
-
- Morrissey DD, Andersen PE, Nesbit GM, Barnwell SL, Everts EC, Cohen JI. Endovascular management of hemorrhage in patients with head and neck cancer. Arch Otolaryngol Head Neck Surg 1997;123:15-19 - PubMed
-
- Borsany SJ. Rupture of the carotids following radical neck surgery in irradiated patients. Ear Nose & Throat Monthly 1962;41:531-533 - PubMed
-
- Ketcham AS, Hoye RC. Spontaneous carotid artery hemorrhage after head and neck surgery. Am J Surg 1965;110:649-655 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources