

Case Reports
Extraorbital inflammatory pseudotumor of the head and neck: CT and MR findings in three patients
Affiliations
- PMID: 10445457
- PMCID: PMC7056226
Item in Clipboard
Case Reports
Extraorbital inflammatory pseudotumor of the head and neck: CT and MR findings in three patients
AJNR Am J Neuroradiol.
1999 Jun-Jul.
Abstract
We review the clinical history and imaging (CT and/or MR) studies in three patients with histologically proved extraorbital inflammatory pseudotumor of the head and neck. The imaging findings in all three cases were nonspecific, mimicking a malignant tumor or granulomatous disease.
Figures
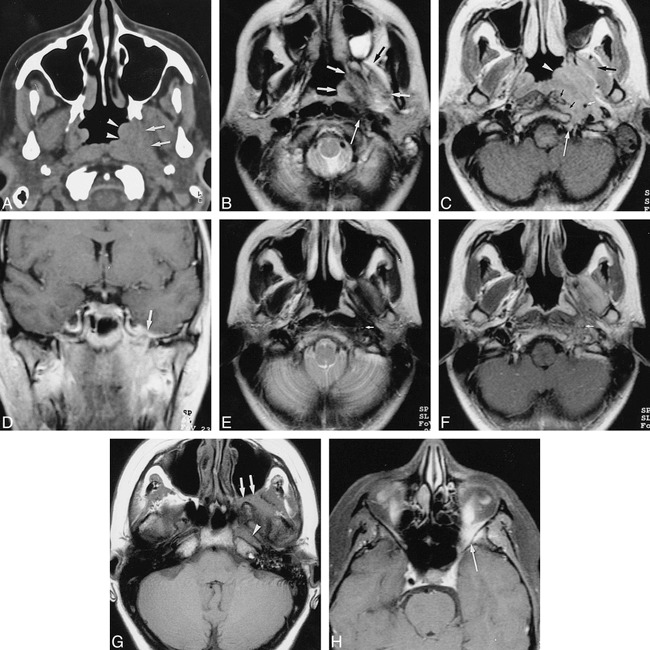
Case 1. A, Unenhanced axial CT scan through the nasopharyngeal region shows thickening of the nasopharyngeal tissues at the level of the left torus tubarius and fossa of Rosenmüller (arrowheads) associated with infiltration of the left parapharyngeal space (arrows). B, Axial T2-weighted MR image through the nasopharyngeal region, obtained 1 month after A. A poorly defined mass lesion (short arrows) is visible in the left nasopharynx and parapharyngeal space. The lateral pterygoid muscle and the origin of the medial pterygoid muscle show high signal intensity, more or less isointense with fat (compare with opposite side). A region of lower signal intensity is also visible within the lesion, extending between the prevertebral muscles and the ICA (long arrow). A left-sided mastoidal effusion is also present. C, Axial contrast-enhanced T1-weighted MR image through the nasopharyngeal region, obtained at same time as B, shows an enhancing soft-tissue mass (arrowhead) in the left nasopharyngeal and retrostyloid compartment of the parapharyngeal space, extending around the left ICA (small white arrow) into the skull base (region of hypoglossal canal, long white arrow), and into the prevertebral muscles (small black arrows). The anterocranial part of the pterygoid muscles also shows some enhancement (large black arrow). D, Coronal contrast-enhanced T1-weighted image, obtained 4 months after B and C, shows further progression of the lesion, now extending up to the foramen ovale with associated enhancement on the floor of the middle cranial fossa (arrow). E and F, Axial T2-weighted (E) and contrast-enhanced T1-weighted (F) images, obtained 4 months after D, after a course of corticosteroids, show the mass lesion is clearly reduced in size. In E, low signal intensity is seen in the left parapharyngeal space, in the fat plane between the lateral pterygoid and temporalis muscle, and around the ICA (arrow). In F, enhancement is visible in and around the left lateral pterygoid muscle and around the left ICA; the normal signal void is not seen in this artery (arrow). G and H, Axial unenhanced (G) and contrast-enhanced fat-suppressed (H) T1-weighted images, obtained 5 months after E and F, when symptoms recurred. The lesion now extends into the left retromaxillary fat and pterygopalatine fossa (arrows, G) and into the orbital apex. Soft-tissue enhancement can be seen posterolaterally in the left orbit (long arrow, H). Absence of normal signal void is evident in the left ICA in the horizontal part of the left carotid canal (arrowhead, G) and in the left cavernous sinus.

Case 2. A, Coronal unenhanced T1-weighted image through the base of the skull. The left pterygopalatine fossa appears infiltrated by soft tissue (thick arrow), isointense with muscle, extending into the inferior orbital fissure (thin arrow). On the opposite side, the pterygopalatine fossa displays its normal high T1 signal intensity, with the internal maxillary artery (arrowhead) visible as a signal void. B and C, Sagittal contrast-enhanced T1-weighted images through the left pterygopalatine fossa: C is 4 mm medial to B. The enhancing mass lesion (arrows, B) is seen to grow through the inferior orbital fissure (white arrow, C) in the orbital apex and into the superior orbital fissure (black arrow, C).
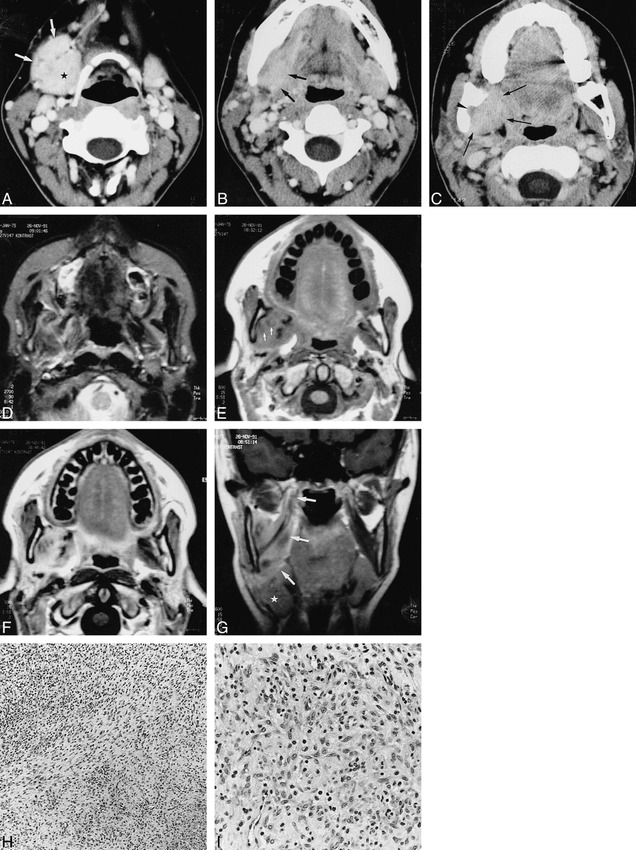
Case 3. A–C, Axial contrast-enhanced CT scans show an enhancing soft-tissue mass (arrows, A) lying against the enlarged and enhancing right submandibular salivary gland (star). At a higher level (B), the mass (arrows) cannot be distinguished from this gland. In C, the soft-tissue mass extends into the medial pterygoid muscle (arrows), abutting the right oropharyngeal wall; there is infiltration of the fat in the mandibular foramen (arrowhead) and associated sclerosis of the mandibular ramus, which appears slightly deformed. D, Axial T2-weighted MR image shows a poorly defined soft-tissue structure, more or less isointense with fat, in the right masticator space. E, Unenhanced T1-weighted image shows that the mass is largely isointense with muscle, with some small low-intensity areas (arrows); some signal loss is evident in the right mandibular ramus. F, After injection of contrast material, there is clear enhancement within the mass, except for the previously indicated low-signal areas, which possibly correspond to areas of fibrosis. G, Coronal T1-weighted image shows the mass infiltrating the medial pterygoid muscle up to its attachment at the skull base (arrows); the submandibular salivary gland is displaced inferiorly (star). H, Low-power histologic section shows spindle cells embedded in a collagenous background and intermingled with mononuclear inflammatory cells (H and E, original magnification ×125). I, At high power, the admixture of the inflammatory cells and the plump (myo)fibroblastlike cells is seen to a better extent (H and E, original magnification ×325).
Similar articles
-
Imaging findings of head and neck inflammatory pseudotumor.AJR Am J Roentgenol. 2009 Oct;193(4):1180-6. doi: 10.2214/AJR.09.2398. AJR Am J Roentgenol. 2009. PMID: 19770345 Review.
-
Head and neck inflammatory pseudotumor: Case series and review of the literature.Neuroradiol J. 2016 Dec;29(6):440-446. doi: 10.1177/1971400916665377. Epub 2016 Sep 20. Neuroradiol J. 2016. PMID: 27650653 Free PMC article. Review.
-
Kimura disease: CT and MR imaging findings.AJNR Am J Neuroradiol. 2012 Apr;33(4):784-8. doi: 10.3174/ajnr.A2854. Epub 2011 Dec 15. AJNR Am J Neuroradiol. 2012. PMID: 22173767 Free PMC article.
-
Pediatric inflammatory pseudotumor of the stomach: contrast-enhanced CT and MR imaging findings.AJR Am J Roentgenol. 1996 Oct;167(4):919-20. doi: 10.2214/ajr.167.4.8819383. AJR Am J Roentgenol. 1996. PMID: 8819383 No abstract available.
-
Unusual CT and MR findings of inflammatory pseudotumor in the parapharyngeal space: case report.AJNR Am J Neuroradiol. 2001 Aug;22(7):1394-7. AJNR Am J Neuroradiol. 2001. PMID: 11498435 Free PMC article.
Cited by
-
[Imaging of nasopharyngeal diseases].HNO. 2009 Aug;57(8):813-24; quiz 825. doi: 10.1007/s00106-009-1966-4. HNO. 2009. PMID: 19639275 Review. German.
-
Malignant tumors and chronic infections in the masticator space: preliminary assessment with in vivo single-voxel 1H-MR spectroscopy.AJNR Am J Neuroradiol. 2008 Apr;29(4):716-9. doi: 10.3174/ajnr.A0897. Epub 2008 Jan 9. AJNR Am J Neuroradiol. 2008. PMID: 18184844 Free PMC article.
-
Is radical surgery necessary to head and neck inflammatory myofibroblastic tumor (IMT) in children?Childs Nerv Syst. 2009 Mar;25(3):285-91. doi: 10.1007/s00381-008-0718-1. Epub 2008 Oct 2. Childs Nerv Syst. 2009. PMID: 18830608 Review.
-
Inflammatory pseudotumor of the head presenting with hemiparesis and aphasia.Case Rep Neurol Med. 2011;2011:176546. doi: 10.1155/2011/176546. Epub 2011 Jul 14. Case Rep Neurol Med. 2011. PMID: 22937331 Free PMC article.
-
Granular cell tumor of the palate: a case report.AJNR Am J Neuroradiol. 2002 May;23(5):850-4. AJNR Am J Neuroradiol. 2002. PMID: 12006292 Free PMC article.
References
-
- Wenig BM, Devaney K, Bisceglia M. Inflammatory myofibroblastic tumor of the larynx: a clinicopathologic study of eight cases simulating a malignant spindle cell neoplasm. Cancer 1995;76:2217-2229 - PubMed
-
- Flanders AE, Mafee MF, Rao VM, Choi KH. CT characteristics of orbital pseudotumors and other orbital inflammatory processes. J Comput Assist Tomogr 1989;13:40-47 - PubMed
-
- Som PM, Brandwein MS, Maldjian C, Reino AJ, Lawson W. Inflammatory pseudotumor of the maxillary sinus: CT and MR findings in six cases. AJR Am J Roentgenol 1994;163:689-692 - PubMed
-
- Keen M, Cho HT, Savetsky L. Pseudotumor of the larynx: an unusual cause of airway obstruction. Otolaryngol Head Neck Surg 1986;94:243-246 - PubMed
-
- Kaye AH, Hahn JF, Craciun A, Hanson M, Berlin AJ, Tubbs RR. Intracranial extension of inflammatory pseudotumor of the orbit. J Neurosurg 1984;60:625-629 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical