

Subtotal versus total gastrectomy for gastric cancer: five-year survival rates in a multicenter randomized Italian trial. Italian Gastrointestinal Tumor Study Group
- PMID: 10450730
- PMCID: PMC1420871
- DOI: 10.1097/00000658-199908000-00006
Subtotal versus total gastrectomy for gastric cancer: five-year survival rates in a multicenter randomized Italian trial. Italian Gastrointestinal Tumor Study Group
Abstract
Objective: To evaluate the impact of subtotal (SG) versus total (TG) gastrectomy on the oncologic outcome of patients with cancer of the distal stomach from 28 Italian institutions.
Summary background data: There is controversy over whether SG and TG have a different impact on the 5-year survival probability of patients with cancer of the distal half of the stomach.
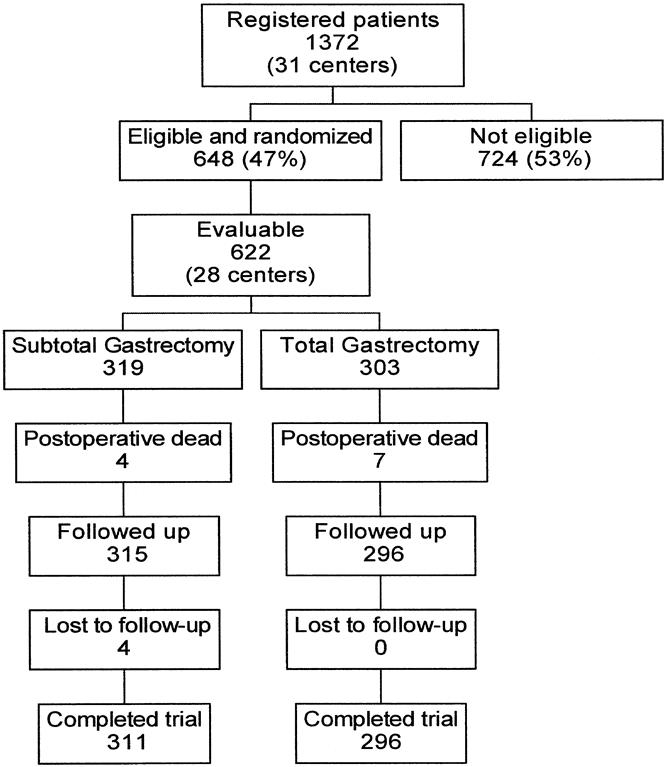
Methods: The present analysis involved 618 patients randomized during surgery to SG (315) or TG (303), provided there was at least 6 cm from the proximal edge of the tumor to the cardia, there was no intrapertoneal or distant spread, and it was possible to remove the tumor entirely. Both surgical treatments included regional lymphadenectomy.
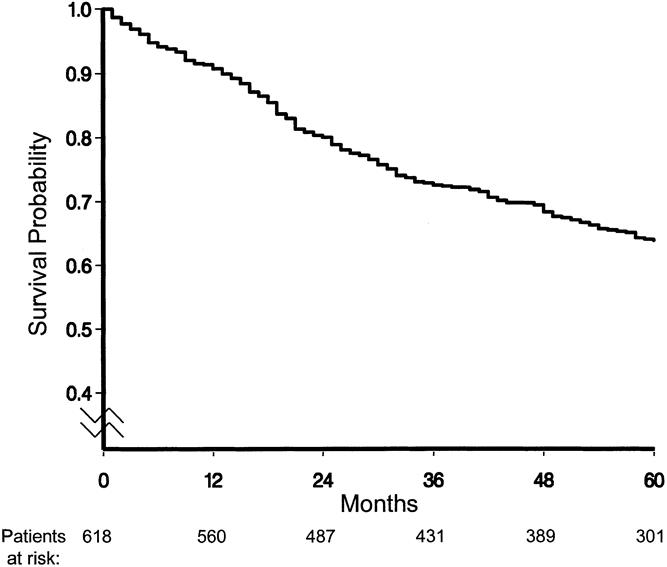
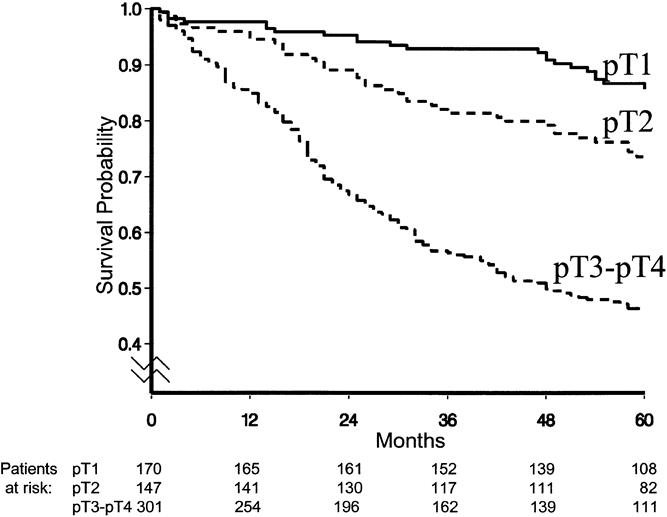
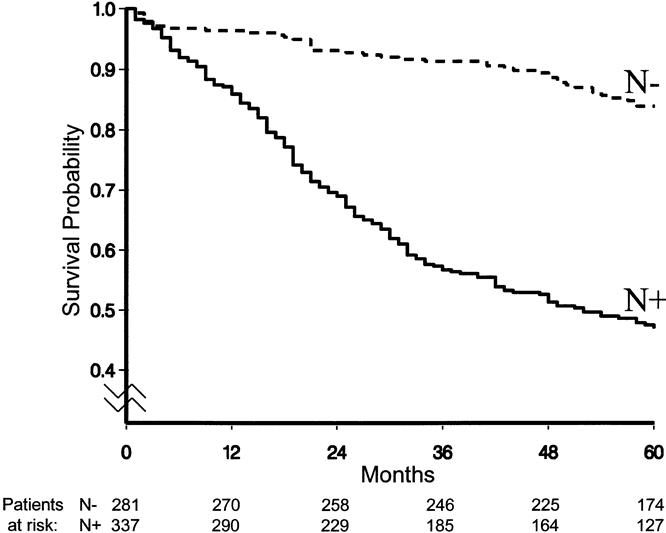
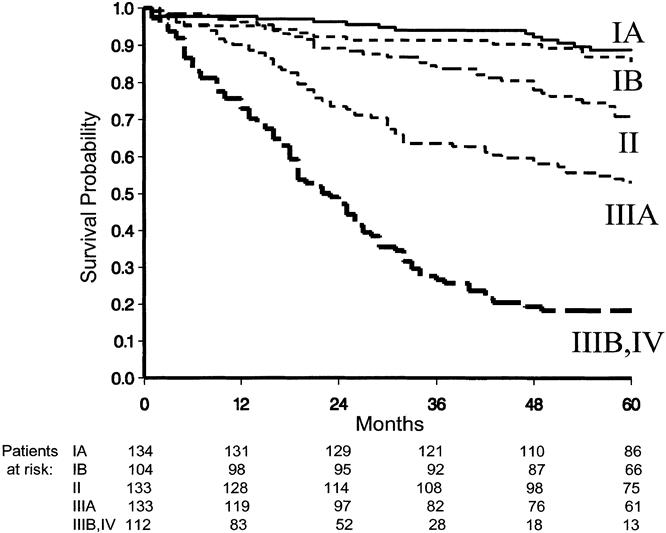
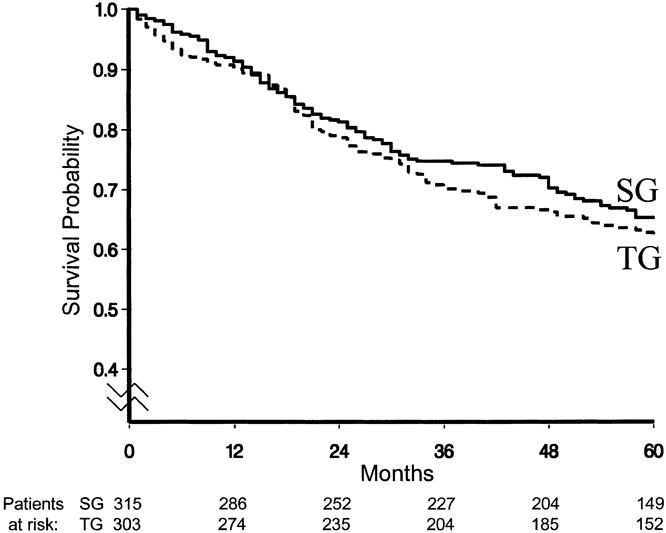
Results: Four patients died after SG and seven after TG. Median follow-up was 72 months after SG (range 2 to 125) and 75 months after TG (range 7 to 113). Five-year survival probability as computed by the Kaplan-Meier method was 65.3% for SG and 62.4% for TG. The test of equivalence led to the conclusion that the two procedures may be considered equivalent in terms of 5-year survival probability. The analysis of survival using a multivariate Cox regression model showed a statistically significant impact on survival of tumor site, tumor spread within the gastric wall, extent of resection to the spleen plus or minus neighboring organs or structures, and relative frequency of metastasis in resected lymph nodes.
Conclusions: Both procedures have a similar survival probability. The authors believe that SG, which has been reported to be associated with a better nutritional status and quality of life, should be the procedure of choice, provided that the proximal margin of the resection falls in healthy tissue.
Figures
References
-
- World Health Organization. The world health report. Geneva: WHO; 1997.
-
- Billroth T. Offenes Schreiben an Herrn Dr. L. Wittelshofer. Wien Med Wochenschr 1881; 31:161–165.
-
- Schlatter K. A unique case of complete removal of the stomach-successful esophago-enterostomy recovery. Med Rec 1897; 52: 909–914.
-
- Heberer G, Teichmann RK, Kramling HJ, Gunther MD. Results of gastric resection for carcinoma of the stomach: The European experience. World J Surg 1988; 12: 374–381. - PubMed
-
- Laurén P. The two histologic main types of gastric carcinoma: Diffuse and so-called intestinal type carcinoma. Acta Path Microbiol Scand 1965; 64: 31–49. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
