

Mechanisms of progression in native coronary artery disease: role of healed plaque disruption
- PMID: 10455072
- PMCID: PMC1729162
- DOI: 10.1136/hrt.82.3.265
Mechanisms of progression in native coronary artery disease: role of healed plaque disruption
Abstract
Objective: To determine the role of healed plaque disruption in the generation of chronic high grade coronary stenosis.
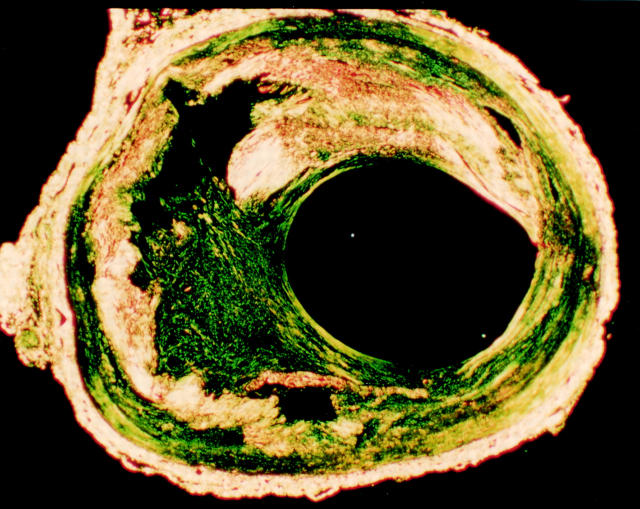
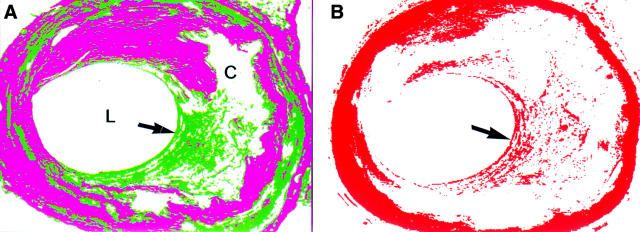
Methods: Coronary arteries obtained at necropsy were perfuse fixed with formal saline for 24 hours at 100 mg Hg. The percentage lumen diameter stenosis was measured in each 3 mm segment containing a plaque, using the lumen size at the nearest histologically normal segment as the reference point. Each segment was prepared for histological examination and stained with Sirius red and immunohistochemistry for smooth muscle actin. Healed disruption was considered to be present when under polarised light there was a break in the yellow-white dense collagen of the cap filled in by more loosely arranged green collagen. Increased smooth muscle density in the green staining areas was required. Each section was read independently by two observers; any segment with discordant views was considered negative.
Material: 31 men aged 51-69 dying suddenly of ischaemic heart disease. 39 coronary arteries were studied containing 256 separate plaques, after excluding coronary arteries with old total occlusions, an acute culprit thrombotic lesion, diffuse disease without normal arterial segments, and arteries related to old myocardial scars.
Results: 16 of 99 plaques causing < 20% diameter stenosis had prior disruption. In the 21-50% stenosis range 16 of 86 plaques showed healed disruption. Stenosis >/= 51% by diameter was present in 71 plaques, 52 of which showed a healed disruption pattern. The difference between stenosis < 50% and stenosis >/= 51% was significant by the chi(2) test (p < 0.001).
Conclusions: Subclinical episodes of plaque disruption followed by healing are a stimulus to plaque growth that occurs suddenly and is a major factor in causing chronic high grade coronary stenosis. This mechanism would explain the phasic rather than linear progression of coronary disease observed in angiograms carried out annually in patients with chronic ischaemic heart disease.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous