

Cost effectiveness of HMG-CoA reductase inhibitor (statin) treatment related to the risk of coronary heart disease and cost of drug treatment
- PMID: 10455083
- PMCID: PMC1729169
- DOI: 10.1136/hrt.82.3.325
Cost effectiveness of HMG-CoA reductase inhibitor (statin) treatment related to the risk of coronary heart disease and cost of drug treatment
Abstract
Objectives: To estimate the cost effectiveness of statin treatment in preventing coronary heart disease (CHD) and to examine the effect of the CHD risk level targeted and the cost of statins on the cost effectiveness of treatment.
Design: Cohort life table method using data from outcome trials.
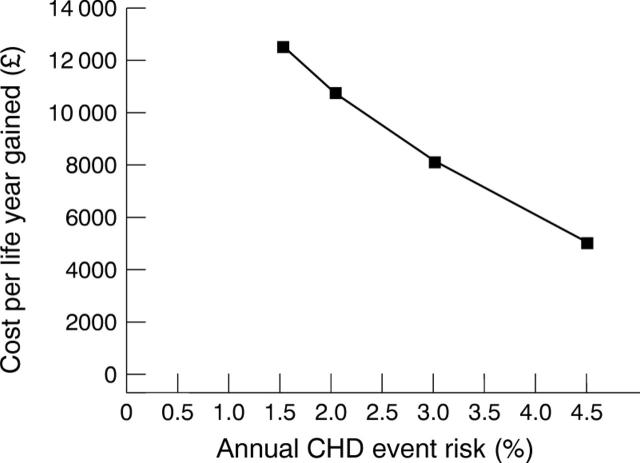
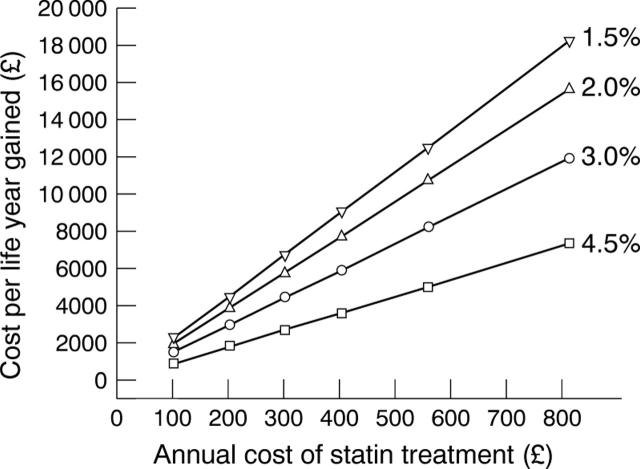
Main outcome measures: The cost per life year gained for lifelong statin treatment at annual CHD event risks of 4.5% (secondary prevention) and 3.0%, 2.0%, and 1.5% (all primary prevention), with the cost of statins varied from pound 100 to pound 800 per year.
Results: The costs per life year gained according to annual CHD event risk were: for 4.5%, pound 5100; 3.0%, pound 8200; 2.0%, pound 10 700; and 1.5%, pound 12 500. Reducing the cost of statins increases cost effectiveness, and narrows the difference in cost effectiveness across the range of CHD event risks.
Conclusions: At current prices statin treatment for secondary prevention, and for primary prevention at a CHD event risk 3.0% per year, is as cost effective as many treatments in wide use. Primary prevention at lower CHD event risks (< 3.0% per year) is less cost effective and unlikely to be affordable at current prices and levels of health service funding. As the cost of statins falls, primary prevention at lower risk levels becomes more cost effective. However, the large volume of treatment needed will remain a major problem.
Figures
Comment in
-
Cost effectiveness of statins.Heart. 2000 Jun;83(6):713-4. doi: 10.1136/heart.83.6.713a. Heart. 2000. PMID: 10885942 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials