

Non-influenza respiratory viruses may overlap and obscure influenza activity
- PMID: 10484251
- PMCID: PMC7166656
- DOI: 10.1111/j.1532-5415.1999.tb05232.x
Non-influenza respiratory viruses may overlap and obscure influenza activity
Erratum in
- J Am Geriatr Soc 1999 Nov;47(11):1363
Abstract
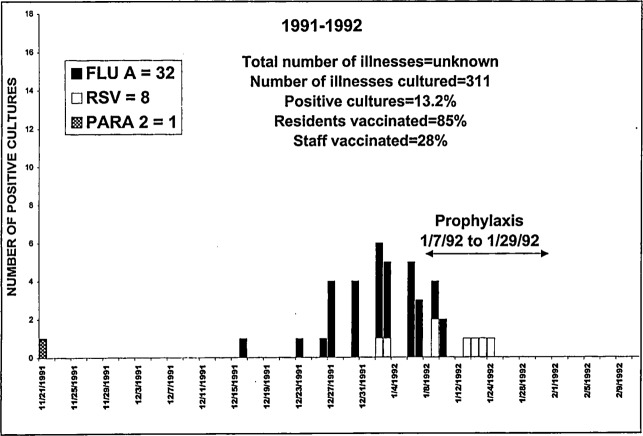
Objective: To report the number and timing of influenza A isolates, as well as overlapping respiratory viruses. Co-circulating respiratory viruses may obscure the determination of influenza activity.
Design: Prospective clinical surveillance for the new onset of respiratory illness followed by viral cultures during seven separate influenza seasons.
Setting: The Wisconsin Veterans Home, a skilled nursing facility for veterans and their spouses.
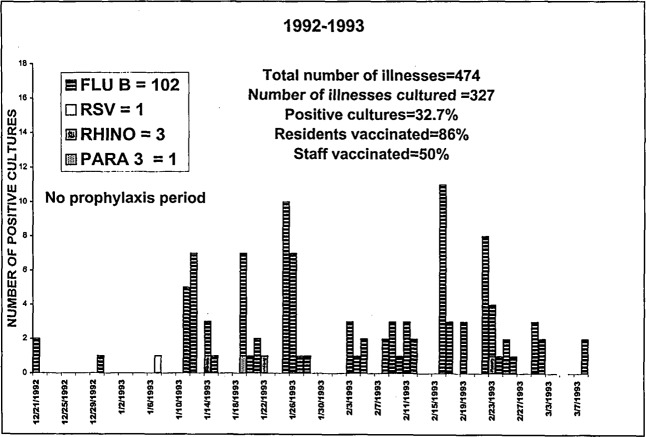
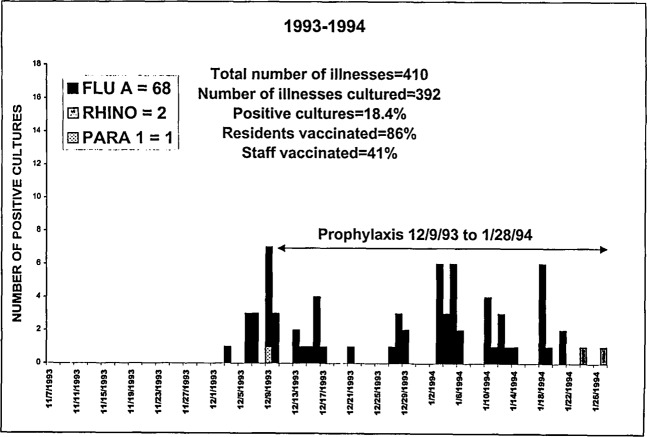
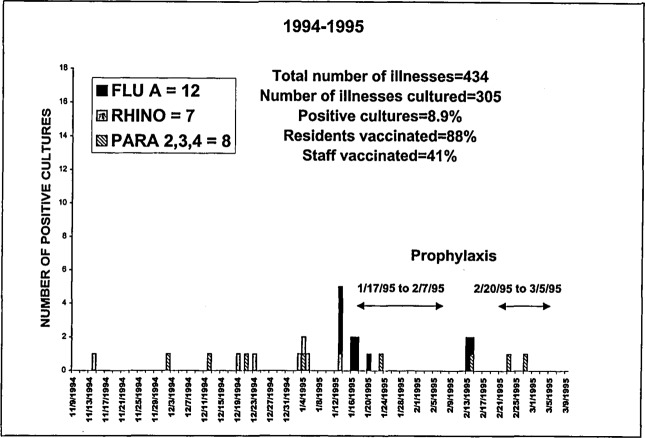
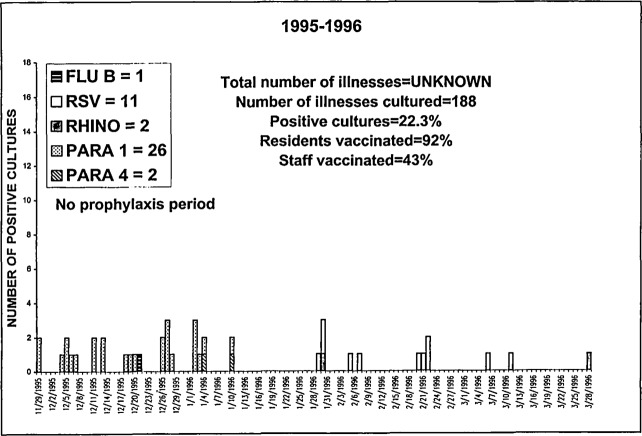
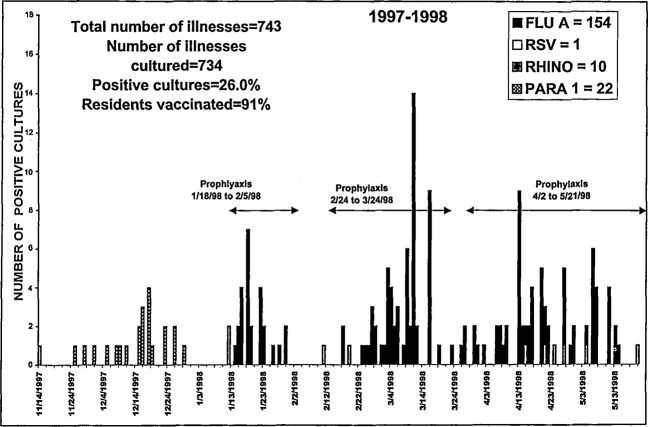
Results: Influenza A isolates were encountered in greater numbers than non-influenza A isolates during three seasons. Seasonal variability is striking. In December 1992, we identified a large outbreak of respiratory illness. Influenza type B was cultured from 102 residents. In December 1995, influenza A was cultured from 285 people in Wisconsin. At that time, we identified outbreaks of respiratory illness in two of our four buildings. Based on statewide data, we suspected an influenza outbreak; however, 26 isolates of parainfluenza virus type 1 were cultured with no influenza. The potential importance of culturing at the end of the season was demonstrated in 1991-1992 when an outbreak of respiratory syncytial virus (RSV) overlapped and extended beyond influenza A activity.
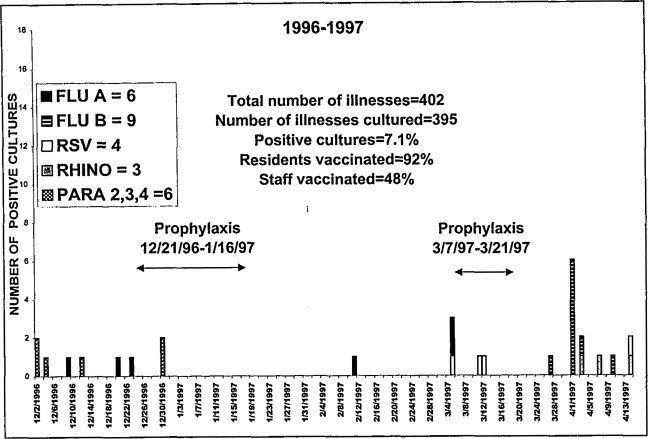
Conclusions: When interpreting new clinical respiratory illnesses as a basis for declaring an outbreak of influenza A, clinicians should realize that co-circulating respiratory viruses can account for clinical illnesses. Clinicians might utilize healthcare dollars efficiently by performing cultures to focus the timing of influenza A chemoprophylaxis. Cultures could be performed when clinical outbreak criteria are approached to confirm an outbreak. Culturing of new respiratory illness could begin again before the anticipated discontinuation of prophylaxis (approximately 2 weeks).
Figures
Similar articles
-
Epidemiologic differences of four major respiratory viruses between children, adolescents, and adults in Korea.J Infect Chemother. 2014 Nov;20(11):672-7. doi: 10.1016/j.jiac.2013.07.009. Epub 2013 Dec 11. J Infect Chemother. 2014. PMID: 25179390
-
Contribution of respiratory syncytial virus, influenza and parainfluenza viruses to acute respiratory infections in San Luis Potosí, Mexico.Pediatr Infect Dis J. 2005 Dec;24(12):1049-52. doi: 10.1097/01.inf.0000190026.58557.93. Pediatr Infect Dis J. 2005. PMID: 16371864
-
Severe acute respiratory infection in children in a densely populated urban slum in Kenya, 2007-2011.BMC Infect Dis. 2015 Feb 25;15:95. doi: 10.1186/s12879-015-0827-x. BMC Infect Dis. 2015. PMID: 25879805 Free PMC article.
-
Global patterns in monthly activity of influenza virus, respiratory syncytial virus, parainfluenza virus, and metapneumovirus: a systematic analysis.Lancet Glob Health. 2019 Aug;7(8):e1031-e1045. doi: 10.1016/S2214-109X(19)30264-5. Lancet Glob Health. 2019. PMID: 31303294
-
Seasonal and pandemic influenza surveillance considerations for constructing multicomponent systems.Influenza Other Respir Viruses. 2009 Mar;3(2):51-8. doi: 10.1111/j.1750-2659.2009.00077.x. Influenza Other Respir Viruses. 2009. PMID: 19496841 Free PMC article. Review.
Cited by
-
What has SARS taught us about infection control in nursing homes?J Am Med Dir Assoc. 2004 Jan-Feb;5(1):59-60. doi: 10.1016/S1525-8610(04)70047-X. J Am Med Dir Assoc. 2004. PMID: 14706132 Free PMC article. Review. No abstract available.
-
Long-term care facilities: a cornucopia of viral pathogens.J Am Geriatr Soc. 2008 Jul;56(7):1281-5. doi: 10.1111/j.1532-5415.2008.01775.x. Epub 2008 Jun 28. J Am Geriatr Soc. 2008. PMID: 18557966 Free PMC article. Clinical Trial.
-
Influenza vaccination and antiviral therapy: is there a role for concurrent administration in the institutionalised elderly?Drugs Aging. 2003;20(3):165-74. doi: 10.2165/00002512-200320030-00001. Drugs Aging. 2003. PMID: 12578397 Review.
-
Current research on respiratory viral infections: Fourth International Symposium.Antiviral Res. 2002 Aug;55(2):227-78. doi: 10.1016/s0166-3542(02)00055-4. Antiviral Res. 2002. PMID: 12103428 Free PMC article. Review. No abstract available.
-
Cationic liposome-mediated enhanced generation of human HLA-restricted RSV-specific CD8+ CTL+.J Clin Immunol. 2002 May;22(3):164-75. doi: 10.1023/a:1015424130339. J Clin Immunol. 2002. PMID: 12078858
References
-
- Advisory Committee on Immunization Practices (ACIP) Prevention and Control of Influenza. Recommendations of the ACIP. MMWR 1998;47:1–26. - PubMed
-
- Gomolin IH, Leib HB, Arden NH, Sherman FT. Control of influenza outbreaks in the nursing home: Guidelines for diagnosis and management. J Am Geriatr Soc 1995;43:71–74. - PubMed
-
- Barker WH, Borisute H, Cox C. A study of the impact of influenza on the functional status of frail older people. Arch Intern Med 1998;158:645–650. - PubMed
-
- Wald TG, Miler BA, Shult P et al. Can respiratory syncytial virus and influenza A be distinguished clinically in institutionalized older persons? J Am Geriatr Soc 1995;43:170–174. - PubMed
-
- Drinka PJ, Gravenstein S, Krause P et al. Outbreaks of influenza A and B in a highly immunized nursing home population. J Fam Pract 1997;45:509–514. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
