

Hospital volume can serve as a surrogate for surgeon volume for achieving excellent outcomes in colorectal resection
- PMID: 10493487
- PMCID: PMC1420885
- DOI: 10.1097/00000658-199909000-00013
Hospital volume can serve as a surrogate for surgeon volume for achieving excellent outcomes in colorectal resection
Abstract
Objective: To examine the association of surgeon and hospital case volumes with the short-term outcomes of in-hospital death, total hospital charges, and length of stay for resection of colorectal carcinoma.
Methods: The study design was a cross-sectional analysis of all adult patients who underwent resection for colorectal cancer using Maryland state discharge data from 1992 to 1996. Cases were divided into three groups based on annual surgeon case volume--low (< or =5), medium (5 to 10), and high (>10)--and hospital volume--low (<40), medium (40 to 70), and high (> or =70). Poisson and multiple linear regression analyses were used to identify differences in outcomes among volume groups while adjusting for variations in type of resections performed, cancer stage, patient comorbidities, urgency of admission, and patient demographic variables.
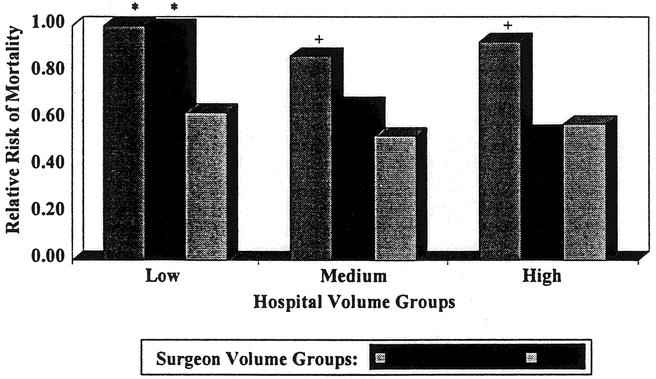
Results: During the 5-year period, 9739 resections were performed by 812 surgeons at 50 hospitals. The majority of surgeons (81%) and hospitals (58%) were in the low-volume group. The low-volume surgeons operated on 3461 of the 9739 total patients (36%) at an average rate of 1.8 cases per year. Higher surgeon volume was associated with significant improvement in all three outcomes (in-hospital death, length of stay, and cost). Medium-volume surgeons achieved results equivalent to high-volume surgeons when they operated in high- or medium-volume hospitals.
Conclusions: A skewed distribution of case volumes by surgeon was found in this study of patients who underwent resection for large bowel cancer in Maryland. The majority of these surgeons performed very few operations for colorectal cancer per year, whereas a minority performed >10 cases per year. Medium-volume surgeons achieved excellent outcomes similar to high-volume surgeons when operating in medium-volume or high-volume hospitals, but not in low-volume hospitals. The results of low-volume surgeons improved with increasing hospital volume but never equaled those of the high-volume surgeons.
Figures
References
-
- Hannan EL, O’Donnell JF, Kilburn H, et al. Investigation of the relationship between volume and mortality for surgical procedures performed in New York State hospitals. JAMA 1989; 262: 503–510. - PubMed
-
- Burns LR, Wholey DR. The effects of patient, hospital, and physician characteristics on length of stay and mortality. Med Care 1991; 29 (3): 251–271. - PubMed
-
- Dardik A, Burleyson GP, Bowman H, et al. Surgical repair of ruptured abdominal aortic aneurysms in the state of Maryland: factors influencing outcome among 527 recent cases. J Vasc Surg 1998; 28 (3): 413–420. - PubMed
-
- Matthews HR, Powell DJ, McConkey CC. Effect of surgical experience on the results of resection for oesophageal carcinoma. Br J Surg 1986; 73: 621–623. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
