

Occult esophageal adenocarcinoma: extent of disease and implications for effective therapy
- PMID: 10493489
- PMCID: PMC1420887
- DOI: 10.1097/00000658-199909000-00015
Occult esophageal adenocarcinoma: extent of disease and implications for effective therapy
Abstract
Objective: The need for esophagectomy in patients with Barrett's esophagus, with no endoscopically visible lesion, and a biopsy showing high-grade dysplasia or adenocarcinoma has been questioned. Recently, endoscopic techniques to ablate the neoplastic mucosa have been encouraged. The aim of this study was to determine the extent of disease present in patients with clinically occult esophageal adenocarcinoma to define the magnitude of therapy required to achieve cure.
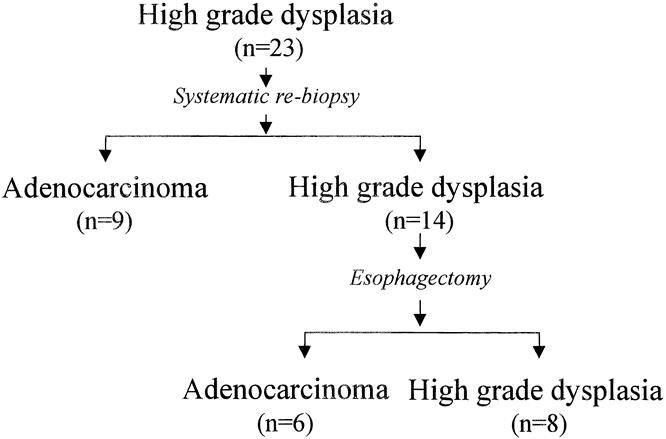
Methods: Thirty-three patients with high-grade dysplasia (23 patients) or adenocarcinoma (10 patients) and no endoscopically visible lesion underwent repeat endoscopy and systematic biopsy followed by esophagectomy. The surgical specimens were analyzed to determine the biopsy error rate in detecting occult adenocarcinoma. In those with cancer, the depth of wall penetration and the presence of lymph node metastases on conventional histology and immunohistochemistry staining was determined. The findings were compared with those in 12 patients (1 with high-grade dysplasia, 11 with adenocarcinoma) who had visible lesions on endoscopy.
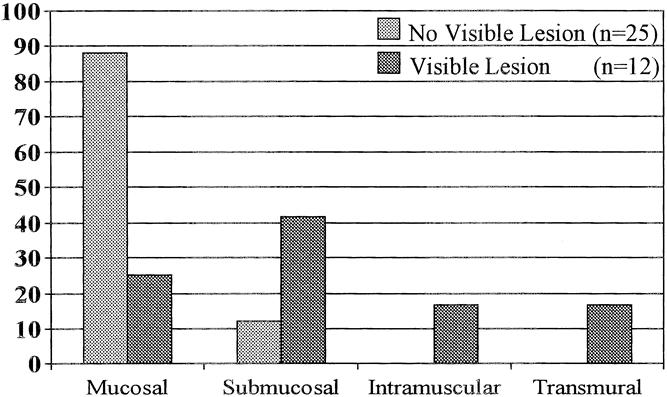
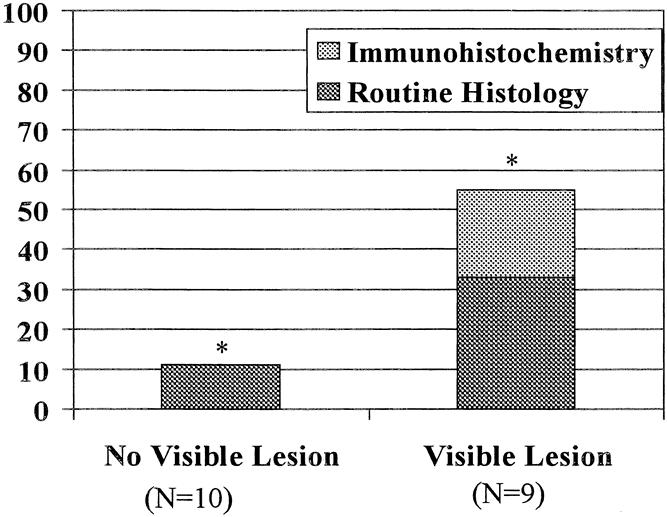
Results: The biopsy error rate for detecting occult adenocarcinoma was 43%. Of 25 patients with cancer and no visible lesion, the cancer was limited to the mucosa in 22 (88%) and to the submucosa in 3 (12%). After en bloc esophagectomy, one patient without a visible lesion had a single node metastasis on conventional histology. No additional node metastases were identified on immunohistochemistry. The 5-year survival rate after esophagectomy was 90%. Patients with endoscopically visible lesions were significantly more likely to have invasion beyond the mucosa (9/12 vs. 3/25, p = 0.01) and involvement of lymph nodes (5/9 vs. 1/10, p = 0.057).
Conclusions: Endoscopy with systematic biopsy cannot reliably exclude the presence of occult adenocarcinoma in Barrett's esophagus. The lack of an endoscopically visible lesion does not preclude cancer invasion beyond the muscularis mucosae, cautioning against the use of mucosal ablative procedures. The rarity of lymph node metastases in these patients encourages a more limited resection with greater emphasis on improved alimentary function (esophageal stripping with vagal nerve preservation) to provide a quality of life compatible with the excellent 5-year survival rate of 90%.
Figures
References
-
- Wang HH, Antonioli DA, Goldman H. Comparative features of esophageal and gastric adenocarcinomas: recent changes in type and frequency. Hum Pathol 1986; 17: 482–487. - PubMed
-
- Hesketh PJ, Clapp RW, Doos WG, Spechler SJ. The increasing frequency of adenocarcinoma of the esophagus. Cancer 1989; 64: 526–530. - PubMed
-
- Hameeteman W, Tytgat, GN, Houthoff HJ, van den Tweel JG. Barrett’s esophagus: development of dysplasia and adenocarcinoma [see comments]. Gastroenterology 1989; 96 (5 Pt 1): 1249–1256. - PubMed
-
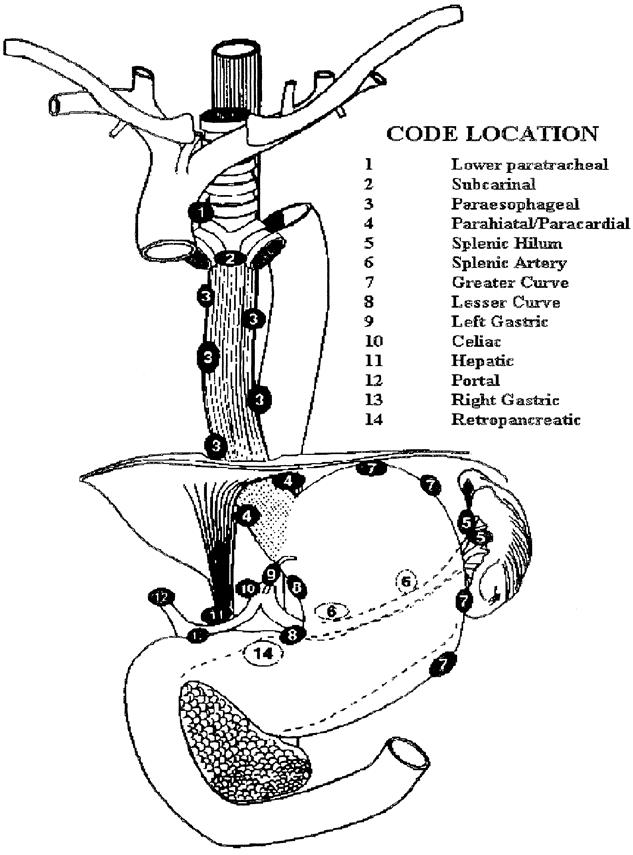
- Hagen JA, Peters JH, DeMeester TR. Superiority of extended en bloc esophagogastrectomy for carcinoma of the lower esophagus and cardia. J Thorac Cardiovasc Sur 1993; 106: 850–859. - PubMed
-
- Riddell RH, Goldman H, Ransohoff DF, et al. Dysplasia in inflammatory bowel disease: standardized classification with provisional clinical applications. Hum Pathol 1983; 14 (11): 931–968. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
