

Hepatic and intestinal transplantation at the University of Pittsburgh
Affiliations
- PMID: 10503105
- PMCID: PMC2956306
Item in Clipboard
Hepatic and intestinal transplantation at the University of Pittsburgh
Clin Transpl.
1998.
No abstract available
Figures

The 4 events that occur in close temporal approximation when there is successful organ engraftment: above, double acute clonal exhaustion (1,2) and subsequent maintenance clonal exhaustion (3) plus, below, loss of organ immunogenicity due to depletion of the graft's passenger leukocytes (4) (From Thomas E. Starzl: The art of tolerance. Nature Med. 1998, 4:1006–1007, used by permission).

Patient and graft survival during the 30-year history of the liver transplantation program at the University of Colorado (1963–1980) and Pittsburgh (1981–1993). The eras were defined by major improvements. The dates of case accrual from bottom to top were 1963–1979 (Group 1), 1980–1989 (Group 2), and 1989–1993 (Group 3). Group 2 and 3 had significantly better survival (p<0.001). AZA =azathioprine, CYA =cyclosporine, FK-506=TAC (From Todo S. Fung J, Starzl TE, et al. Single-center experience with primary orthotopic liver transplantation with FK-506 immunosuppression. Ann of Surg, 1994: 220, 297–309.

The cumulative survival of the first 1,000 consecutive patients who received primary liver transplantation under TAC-based immunosuppression.

The Kaplan-Meier patient (A) and graft (B) survival according to age.
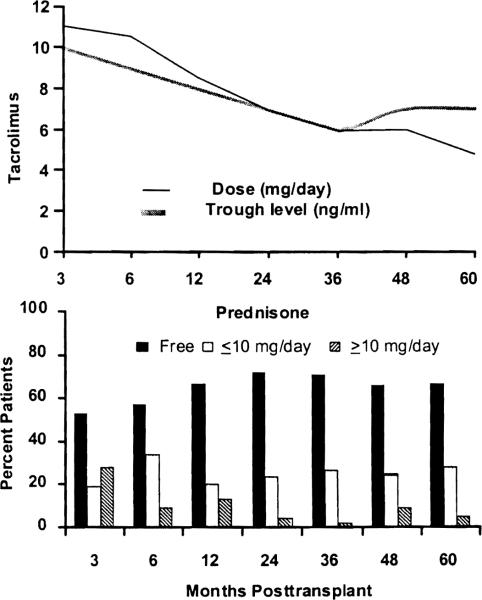
The TAC dose, drug trough level, and prednisone dose during the first 5 years after liver transplantation.

Frequency of distribution of various malignancies among liver recipients treated with TAC compared with the general population (From Jain AB, Yee LD, Nalesnik MA, et al: Comparative incidence of de novo nonlymplzoid malignancies after liver transplantation under TAC using surveillance epidemiologic end result data. Transplantation 1998, 66:1193–1200, used by permission).

Kaplan-Meier actuarial patient (A) and graft (B) survival curves for TAC and steroids (double) therapy versus TAC, steroids and mycophenolate mofetil (triple) therapy.

The yearly cumulative increase in the patient survival at one, 2 and 5 years after liver transplantation at the University of Pittsburgh during the last 15 years.

The results of the weaning trial among the pediatric and adult population (From Mazariegos GV, Reyes J, Marino IR, et al: Weaning of immunosuppression in liver transplant recipients. Transplantation 1997, 63:243–249, used by permission).

The effect of the baseline immunosuppression on the cumulative rate of complete drug withdrawal (From Mazariegos GV, Reyes J, Marino IR, et al: Weaning of immunosuppression in liver transplant recipients. Transplantation 1997, 63:243–249, used by permission).

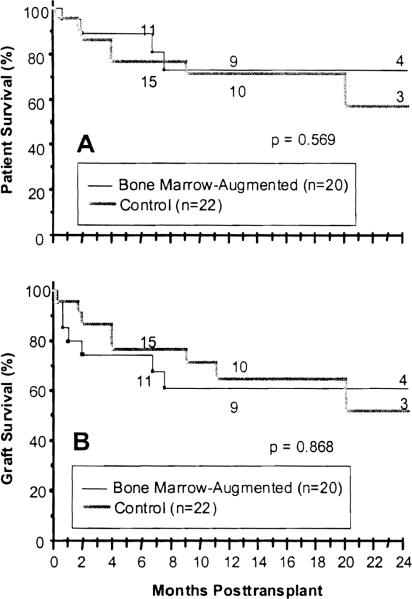
The actuarial graft (A) and patient (B) survival in bone marrow-augmented and control organ allograft recipients. Bone marrow augmentation was with either single or multiple infusions (From Rao As, Shapiro R, Corry R, et al: Adjuvant bone marrow infusion in clinical organ transplant recipients. Transplant Proc 1998, 30: 1367–1368, used by permission).

The cumulative risk of acute cellular rejection in the study versus the control group (A), and with single versus multiple bone marrow infusions (B) (From Salgar S, Shapiro R, Dodson F, et al: Infusion of donor leukocytes to induce tolerance in organ allograft recipients. J Leukocyte Biology, In Press, used by permission).

The actuarial patient (A) and graft (B) survival after liver transplantation for the hepatitis C patients and control (non-viral and non-malignant liver disease) group (From Casavilla A, Rakela J, Kapur S, et al: Clinical outcome of patients infected with hepatitis C virus infection on survival after primary liver transplantation under TAC. Liver Transplantation and Surgery 1998, 4:448–454, used by permission).

The cumulative risk of primary graft loss among the HCV liver recipients and control group (From Casavilla A, Rakela J, Kapur S, et al: Clinical outcome of patients infected with hepatitis C virus infection on survival after primary liver transplantation under TAC. Liver Transplantation and Surgery 1998, 4:448–454, used by permission).

The effect of postoperative chemotherapy on the cumulative survival of the HCC patients who were at high risk of tumor recurrence after liver transplantation (From Marsh JW, Dvorchik I, Subotin M, et al: The prediction of risk of recurrence and time to recurrence of hepatocellular carcinoma after orthotopic liver transplantation: A pilot study. Hepatology 1997, 26:444–450, used by permission).

Composite liver and intestinal graft with preservation of the duodenum in continuity with the graft jejunum and hepatic biliary system (From Abu-Elmagd K, Reyes J, Todo S, et al: Clinical intestinal transplantation: New perspectives and immunologic considerations. J Am Coll Surg 1998, 186:512–527, used by permission).

Kaplan-Meier patient and graft survival rates for the total intestinal allograft recipients (From Abu-Elmagd K, Reyes J, Todo S, et al: Clinical intestinal transplantation: New perspectives and immunologic considerations. J Am Coll Surg 1998, 186:512–527, used by permission).

The cumulative survival of the composite grafts that contained liver and the intestine only (From Abu-Elmagd K, Reyes J, Todo S, et al: Clinical intestinal transplantation: New perspectives and immunologic considerations. J Am Coll Surg 1998, 186:512–527, used by permission).
Patient (A) and graft (B) survival rates for the bone marrow-augmented and control groups (From Abu-Elmagd K, Reyes J, Todo S, et al: Clinical intestinal transplantation: New perspectives and immunologic considerations. J Am Coll Surg 1998, 186:512–527, used by permission).

The cumulative risk of intestinal rejection (A), and graft loss from rejection (B) for both the isolated intestine and composite grafts that contained liver (From Abu-Elmagd K, Reyes J, Todo S, et al: Clinical intestinal transplantation: New perspectives and immunologic considerations. J Am Coll Surg 1998, 186:512–527, used by permission).

Cumulative risk of both intestinal and hepatic rejection in the composite visceral allografts (From Abu-Elmagd K, Reyes J, Todo S, et al: Clinical intestinal transplantation: New perspectives and immunologic considerations. J Am Coll Surg 1998, 186:512–527, used by permission).

Graft survival before and after the 1994 moratorium (From Abu-Elmagd K, Reyes, Fung JJ, et al: Evolution of clinical intestinal transplantation: Improved outcome and cost effectiveness. Transplant Proc, in Press, used by permission).
Similar articles
-
Clinical outcome of intestinal transplantation at the University of Miami.Transplant Proc. 1999 Feb-Mar;31(1-2):569-71. doi: 10.1016/s0041-1345(98)01558-9. Transplant Proc. 1999. PMID: 10083240 No abstract available.
-
Mycophenolate mofetil as primary and rescue therapy in intestinal transplantation.Transplant Proc. 1998 Sep;30(6):2677-9. doi: 10.1016/s0041-1345(98)00786-6. Transplant Proc. 1998. PMID: 9745545 No abstract available.
-
Status of liver and gastrointestinal transplantation at the University of Miami.Clin Transpl. 1996:187-201. Clin Transpl. 1996. PMID: 9286568
-
The current status of hepatic transplantation at the University of Pittsburgh.Clin Transpl. 1995:145-70. Clin Transpl. 1995. PMID: 8794262 Free PMC article. Review.
-
Pediatric transplantation.Am J Transplant. 2004;4 Suppl 9:54-71. doi: 10.1111/j.1600-6143.2004.00398.x. Am J Transplant. 2004. PMID: 15113355 Review.
Cited by
-
Immunomodulation for intestinal transplantation by allograft irradiation, adjunct donor bone marrow infusion, or both.Transplantation. 2000 Dec 15;70(11):1632-41. doi: 10.1097/00007890-200012150-00016. Transplantation. 2000. PMID: 11152226 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical