

Assessment of functional MR imaging in neurosurgical planning
- PMID: 10512239
- PMCID: PMC7657751
Assessment of functional MR imaging in neurosurgical planning
Abstract
Background and purpose: Presurgical sensorimotor mapping with functional MR imaging is gaining acceptance in clinical practice; however, to our knowledge, its therapeutic efficacy has not been assessed in a sizable group of patients. Our goal was to identify how preoperative sensorimotor functional studies were used to guide the treatment of neuro-oncologic and epilepsy surgery patients.
Methods: We retrospectively reviewed the medical records of 46 patients who had undergone preoperative sensorimotor functional MR imaging to document how often and in what ways the imaging studies had influenced their management. Clinical management decisions were grouped into three categories: for assessing the feasibility of surgical resection, for surgical planning, and for selecting patients for invasive functional mapping procedures.
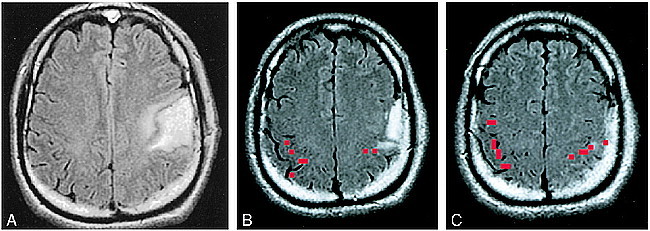
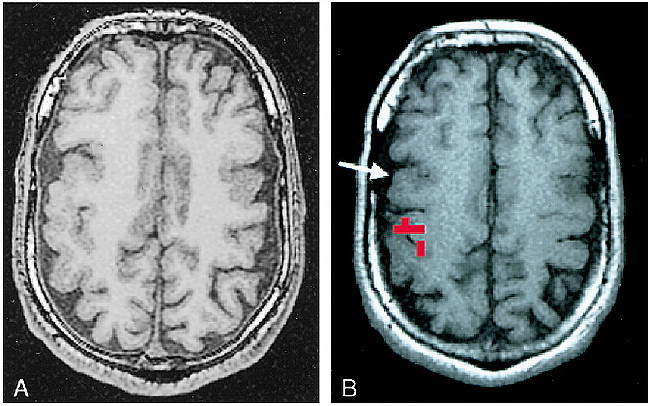
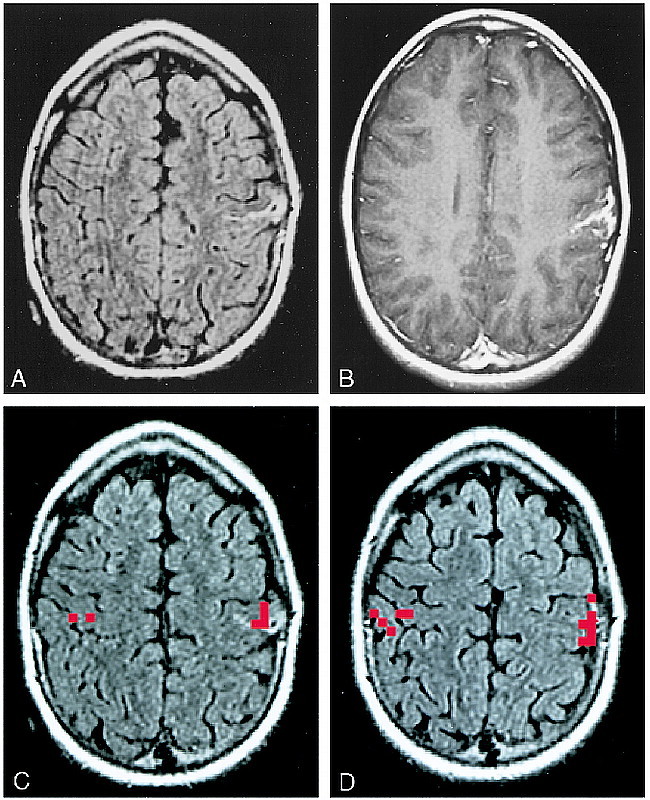
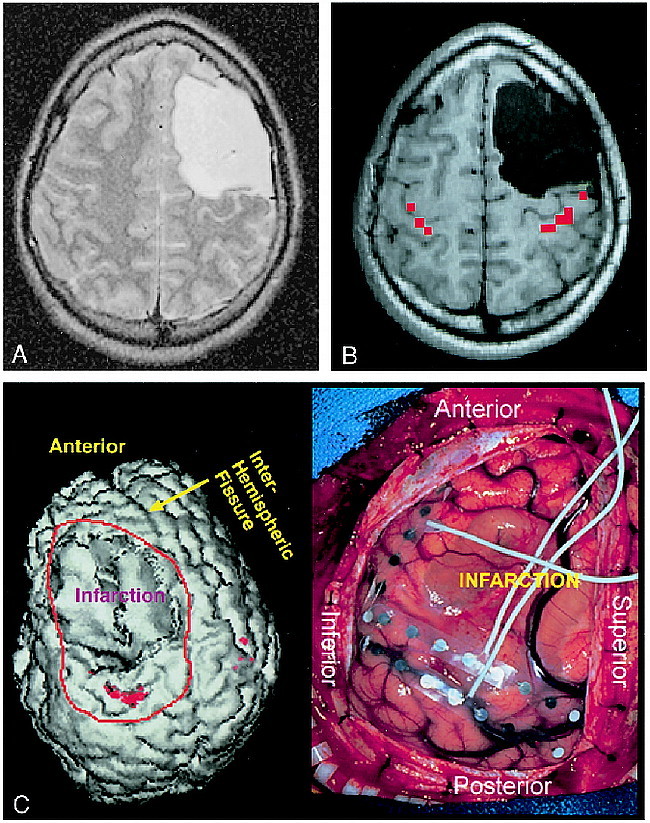
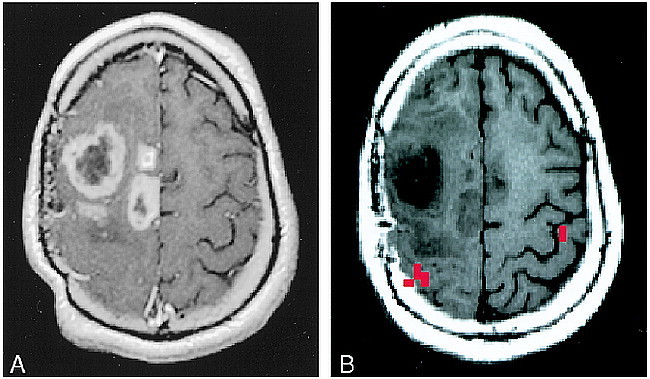
Results: Functional MR imaging studies successfully identified the functional central sulcus ipsilateral to the abnormality in 32 of the 46 patients, and these 32 patients are the focus of this report. In epilepsy surgery candidates, the functional MR imaging results were used to determine in part the feasibility of a proposed surgical resection in 70% of patients, to aid in surgical planning in 43%, and to select patients for invasive surgical functional mapping in 52%. In tumor patients, the functional MR imaging results were used to determine in part the feasibility of surgical resection in 55%, to aid in surgical planning in 22%, and to select patients for invasive surgical functional mapping in 78%. Overall, functional MR imaging studies were used in one or more of the three clinical decision-making categories in 89% of tumor patients and 91% of epilepsy surgery patients.
Conclusion: Preoperative functional MR imaging is useful to clinicians at three key stages in the preoperative clinical management paradigm of a substantial percentage of patients who are being considered for resective tumor or epilepsy surgery.
Figures
References
-
- Skirboll SS, Ojemann GA, Berger MS,, et al. Functional cortex and subcortical white matter located within gliomas. . Neurosurgery 1996;38:678-685 - PubMed
-
- Woolsey CN, Erickson TC, Gilson WE. Localization in somatic sensory and motor areas of human cerebral cortex as determined by direct recording of evoked potentials and electrical stimulation. . J Neurosurg 1979;51:476-506 - PubMed
-
- Ojemann GA, Sutherling WW, Lesser RP,, et al. Cortical stimulation. . In: Engel JJ, ed. Surgical Treatment of the Epilepsies. New York: Raven Press; 1993;399-414
-
- Gregorie EM, Goldring S. Localization of function in the excision of lesions from the sensorimotor region. . J Neurosurg 1984;61:1047-1054 - PubMed
-
- Berger MS, Cohen WA, Ojemann GA. Correlation of motor cortex brain mapping data with magnetic resonance imaging. . J Neurosurg 1990;72:383-387 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical