

Q fever
- PMID: 10515901
- PMCID: PMC88923
- DOI: 10.1128/CMR.12.4.518
Q fever
Abstract
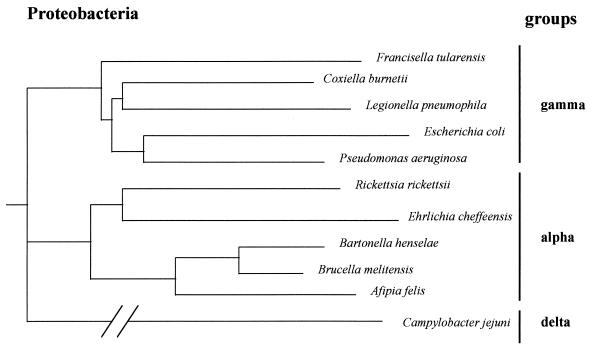
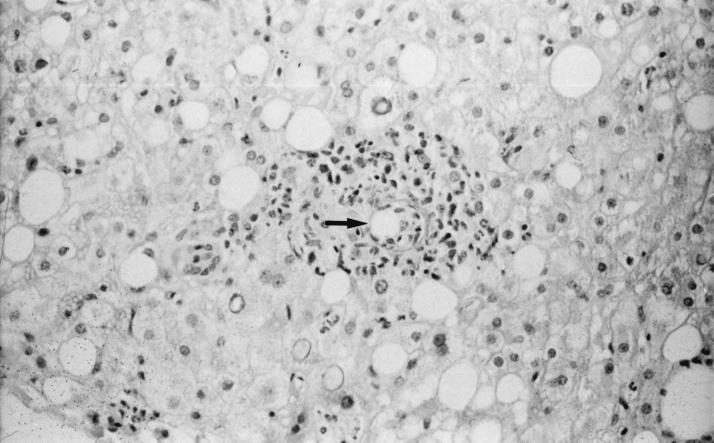
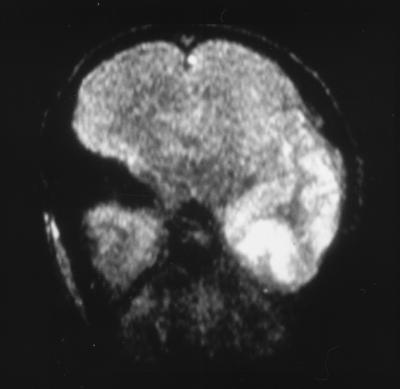
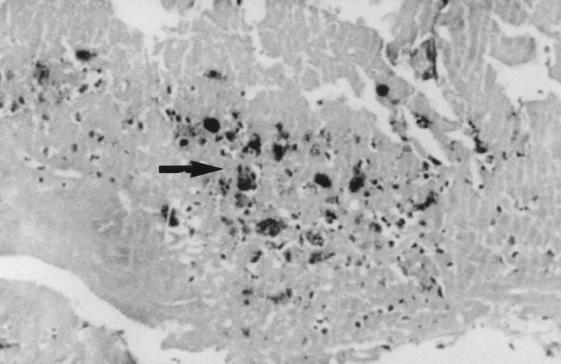
Q fever is a zoonosis with a worldwide distribution with the exception of New Zealand. The disease is caused by Coxiella burnetii, a strictly intracellular, gram-negative bacterium. Many species of mammals, birds, and ticks are reservoirs of C. burnetii in nature. C. burnetii infection is most often latent in animals, with persistent shedding of bacteria into the environment. However, in females intermittent high-level shedding occurs at the time of parturition, with millions of bacteria being released per gram of placenta. Humans are usually infected by contaminated aerosols from domestic animals, particularly after contact with parturient females and their birth products. Although often asymptomatic, Q fever may manifest in humans as an acute disease (mainly as a self-limited febrile illness, pneumonia, or hepatitis) or as a chronic disease (mainly endocarditis), especially in patients with previous valvulopathy and to a lesser extent in immunocompromised hosts and in pregnant women. Specific diagnosis of Q fever remains based upon serology. Immunoglobulin M (IgM) and IgG antiphase II antibodies are detected 2 to 3 weeks after infection with C. burnetii, whereas the presence of IgG antiphase I C. burnetii antibodies at titers of >/=1:800 by microimmunofluorescence is indicative of chronic Q fever. The tetracyclines are still considered the mainstay of antibiotic therapy of acute Q fever, whereas antibiotic combinations administered over prolonged periods are necessary to prevent relapses in Q fever endocarditis patients. Although the protective role of Q fever vaccination with whole-cell extracts has been established, the population which should be primarily vaccinated remains to be clearly identified. Vaccination should probably be considered in the population at high risk for Q fever endocarditis.
Figures

References
-
- Ackland J R, Worswick D A, Marmion B P. Vaccine prophylaxis of Q fever. A follow-up study of the efficacy of Q-Vax (CSL) 1985–1990. Med J Aust. 1994;160:704–708. - PubMed
-
- Aitken I D, Bögel K, Cracea E, Edlinger E, Houwers D, Krauss H, Rady M, Rehacek J, Schiefer H G, Schmeer N, Tarasevich I V, Tringali G. Q fever in Europe: current aspects of aetiology, epidemiology, human infection, diagnosis and therapy. Infection. 1987;15:323–327. - PubMed
-
- Aitken I D. Clinical aspects and prevention of Q fever in animals. Eur J Epidemiol. 1989;5:420–424. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
