

Alcohol interventions in a trauma center as a means of reducing the risk of injury recurrence
- PMID: 10522717
- PMCID: PMC1420896
- DOI: 10.1097/00000658-199910000-00003
Alcohol interventions in a trauma center as a means of reducing the risk of injury recurrence
Abstract
Objective: Alcoholism is the leading risk factor for injury. The authors hypothesized that providing brief alcohol interventions as a routine component of trauma care would significantly reduce alcohol consumption and would decrease the rate of trauma recidivism.
Methods: This study was a randomized, prospective controlled trial in a level 1 trauma center. Patients were screened using a blood alcohol concentration, gamma glutamyl transpeptidase level, and short Michigan Alcoholism Screening Test (SMAST). Those with positive results were randomized to a brief intervention or control group. Reinjury was detected by a computerized search of emergency department and statewide hospital discharge records, and 6- and 12-month interviews were conducted to assess alcohol use.
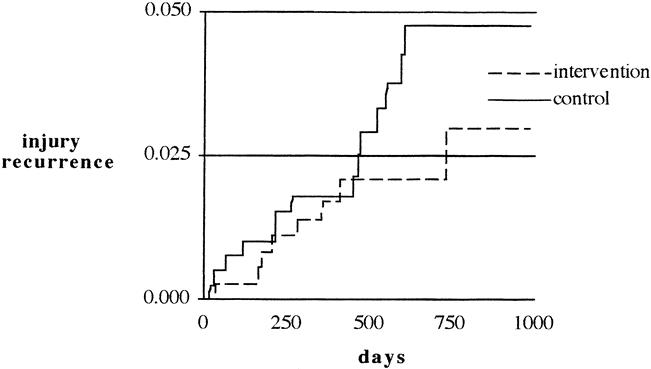
Results: A total of 2524 patients were screened; 1153 screened positive (46%). Three hundred sixty-six were randomized to the intervention group, and 396 to controls. At 12 months, the intervention group decreased alcohol consumption by 21.8+/-3.7 drinks per week; in the control group, the decrease was 6.7+/-5.8 (p = 0.03). The reduction was most apparent in patients with mild to moderate alcohol problems (SMAST score 3 to 8); they had 21.6+/-4.2 fewer drinks per week, compared to an increase of 2.3+/-8.3 drinks per week in controls (p < 0.01). There was a 47% reduction in injuries requiring either emergency department or trauma center admission (hazard ratio 0.53, 95% confidence interval 0.26 to 1.07, p = 0.07) and a 48% reduction in injuries requiring hospital admission (3 years follow-up).
Conclusion: Alcohol interventions are associated with a reduction in alcohol intake and a reduced risk of trauma recidivism. Given the prevalence of alcohol problems in trauma centers, screening, intervention, and counseling for alcohol problems should be routine.
Figures




References
-
- West J, Trunkey DD, Lim RC. Systems of trauma care:: a study of two counties. Arch Surg 1979; 114: 497–501. - PubMed
-
- Cales RH. Trauma mortality in Orange County: : the effect of implementation of a regional trauma system. Ann Emerg Med 1984; 13: 1–10. - PubMed
-
- Baker CC, Oppenheimer L, Stephens B, Lewis FR, Trunkey DD. Epidemiology of trauma deaths. Am J Surg 1980; 140: 144–150. - PubMed
-
- Sauaia A, Moore FA, Moore EE, et al. Epidemiology of trauma deaths:: a reassessment. J Trauma 1995; 38: 185–193. - PubMed
-
- Gentilello LM, Donovan DM, Dunn C, Rivara FP. Alcohol interventions in level 1 trauma centers: : current practice, future directions. JAMA 1995; 274: 1043–1048. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
