

Safety and efficacy of low anterior resection for rectal cancer: 681 consecutive cases from a specialty service
- PMID: 10522724
- PMCID: PMC1420903
- DOI: 10.1097/00000658-199910000-00010
Safety and efficacy of low anterior resection for rectal cancer: 681 consecutive cases from a specialty service
Abstract
Objective: To determine perioperative morbidity, survival, and local failure rates in a large group of consecutive patients with rectal cancer undergoing low anterior resection by multiple surgeons on a specialty service. The primary objective was to assess the surgical complications associated with preoperative radiation sequencing.
Summary background data: The goals in the treatment of rectal cancer are cure, local control, and preservation of sphincter, sexual, and bladder function. Surgical resection using sharp perimesorectal dissection is important for achieving these goals. The complications and mortality rate of this surgical strategy, particularly in the setting of preoperative chemoradiation, have not been well defined.
Methods: There were 1233 patients with primary rectal cancer treated at the authors' cancer center from 1987 to 1995. Of these, 681 underwent low anterior resection and/or coloanal anastomosis for primary rectal cancer. The surgical technique used the principles of sharp perimesorectal excision. Morbidity and mortality rates were compared between patients receiving preoperative chemoradiation (Preop RT, n = 150) and those not receiving preoperative chemoradiation (No Preop RT, n = 531). Recurrence and survival data were determined in patients undergoing curative resection (n = 583, 86%) among three groups of patients: those receiving Preop RT (n = 131), those receiving postoperative chemoradiation (Postop RT, n = 110), and those receiving no radiation therapy (No RT, n = 342).
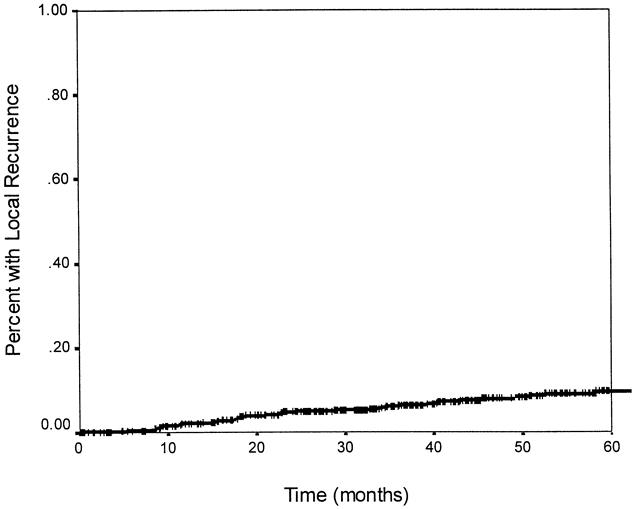
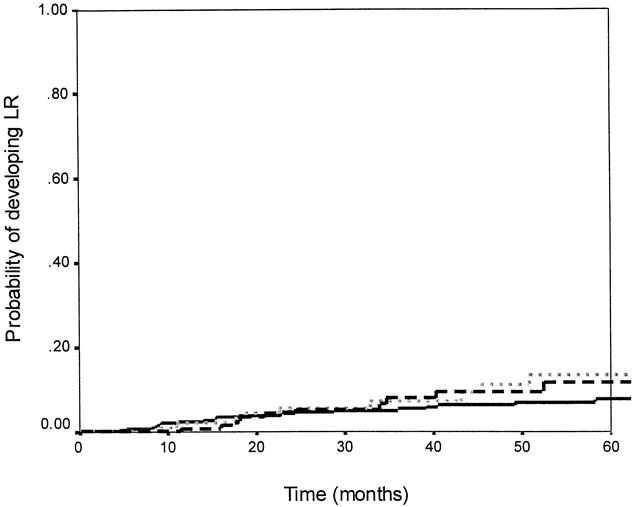
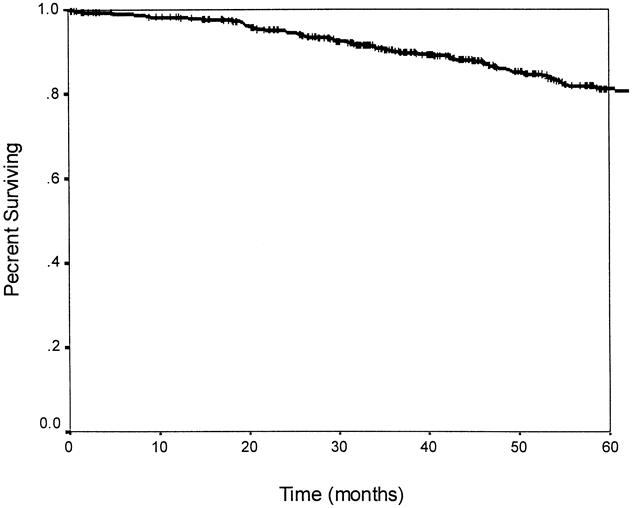
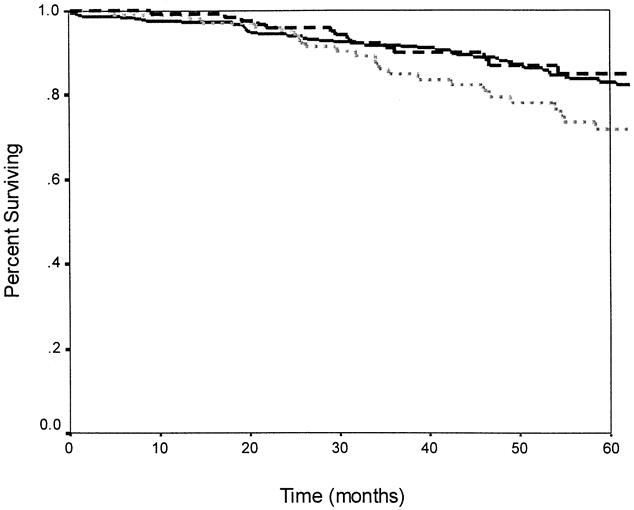
Results: The perioperative mortality rate was 0.6% (4/681). Postoperative complications occurred in 22% (153/681). The operative time, estimated blood loss, and rate of pelvic abscess formation without associated leak were higher in the Preop RT group than the No Preop RT group. However, the overall complication rate, rate of wound infection, anastomotic leak, and length of hospital stay were no different between Preop RT and No Preop RT patients. With a median follow-up of 45.6 months, the overall actuarial 5-year recurrence rate for patients undergoing curative resection (n = 583) was 19%, with 4% having local recurrence only, 12% having distant recurrence, and 3% having both local and distant recurrence, for an overall local recurrence rate of 7%. The actuarial 5-year overall survival rate was 81%; the disease-free survival rate was 75% and the local recurrence rate was 10%. The overall survival rate was similar between Preop RT (85%), Postop RT (72%), and No RT (83%) patients (p = 0.10), whereas the disease-free survival rate was significantly worse for Postop RT (65%) patients compared with Preop RT (79%) and No RT (77%) patients (p = 0.04).
Conclusion: The use of preoperative chemoradiation results in increased operative time, blood loss, and pelvic abscess formation but does not increase the rate of anastomotic leaks or the length of hospital stay after low anterior resection for rectal cancer. The 5-year actuarial overall survival rate for patients undergoing curative resection exceeded 80%, with a local recurrence rate of 10%.
Figures
References
-
- Cohen A, Minsky B, Schlisky RL. Cancer of the rectum. In: DeVita V, Hellman S, Rosenberg SA, eds. Cancer: principles and practice of oncology, 5th ed. Philadelphia: Lippincott-Raven; 1997.
-
- Pilipshen SJ, Heilweil M, Quan SH, Sternberg SS, Enker WE. Patterns of pelvic recurrence following definitive resections of rectal cancer. Cancer 1984; 53: 1354–1362. - PubMed
-
- Minsky BD, Mies C, Recht A, Rich TA, Chaffey JT. Resectable adenocarcinoma of the rectosigmoid and rectum. I. Patterns of failure and survival. Cancer 1988; 61: 1408–1416. - PubMed
-
- Gastrointestinal Tumor Study Group. Prolongation of the disease-free interval in surgically treated rectal carcinoma. N Engl J Med 1985; 312: 1465–1472. - PubMed
-
- Krook JE, Moertel CG, Gunderson LL, et al. Effective surgical adjuvant therapy for high-risk rectal carcinoma. N Engl J Med 1991; 324: 709–715. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
