

Clinical and pathologic predictors of survival in patients with thymoma
- PMID: 10522726
- PMCID: PMC1420905
- DOI: 10.1097/00000658-199910000-00012
Clinical and pathologic predictors of survival in patients with thymoma
Abstract
Objective: To evaluate the Johns Hopkins Hospital experience with 136 thymomas over the past 40 years. This number of patients allowed quantitative estimation of the independent influence of common clinicopathologic risk factors using multivariate analysis.
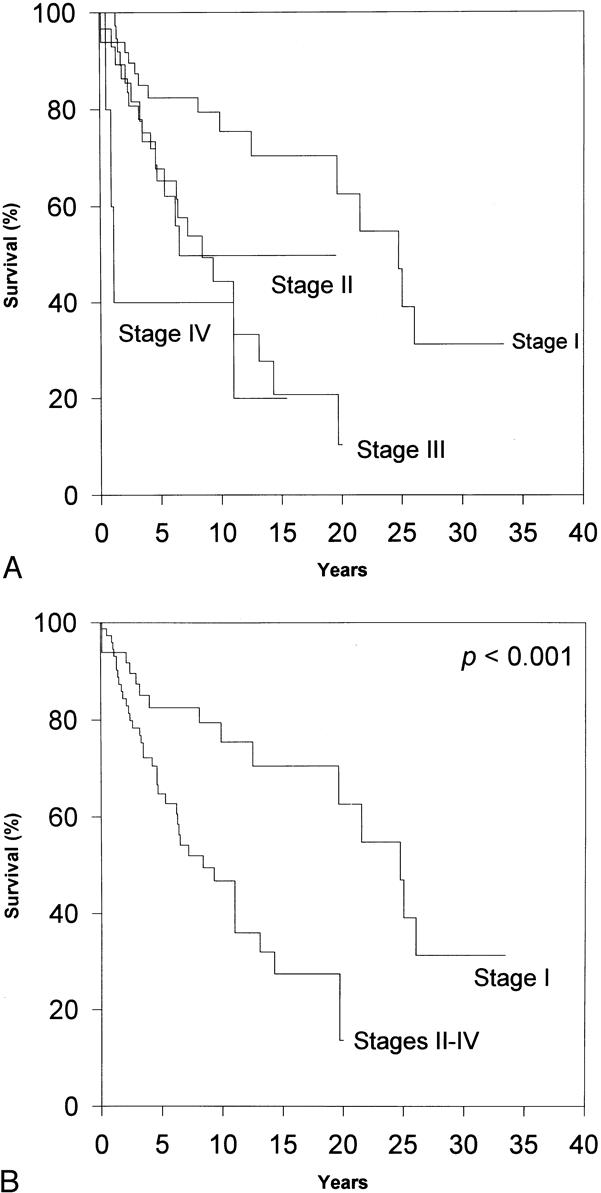
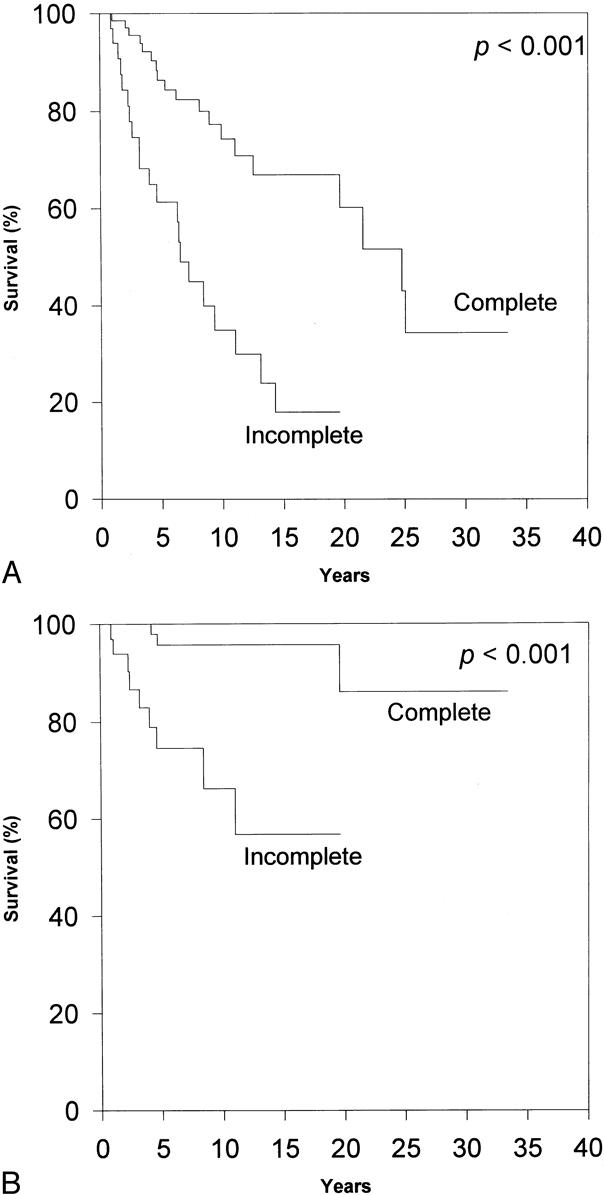
Summary background data: Thymomas vary widely in terms of recurrence and influence on overall survival. Several series have indicated the importance of initial tumor invasion, as well as the extent of surgical resection, as predictors of recurrence and survival after thymoma resection. However, findings have been equivocal when other predictors of prognosis were examined.
Methods: The authors evaluated 136 patients seen at the Johns Hopkins Hospital between 1957 and 1997 with a pathologic diagnosis of thymoma. Demographic information, clinical staging data, surgical and adjuvant treatment details, and patient follow-up data were obtained from the patient record and from detailed patient or family interviews. Microscopic sections of all 136 patients were reviewed by two pathologists blinded to the clinical data. All data were analyzed by multivariate Cox regression analysis, which allowed the quantification of the independent predictive value of 12 putative clinicopathologic prognostic indicators.
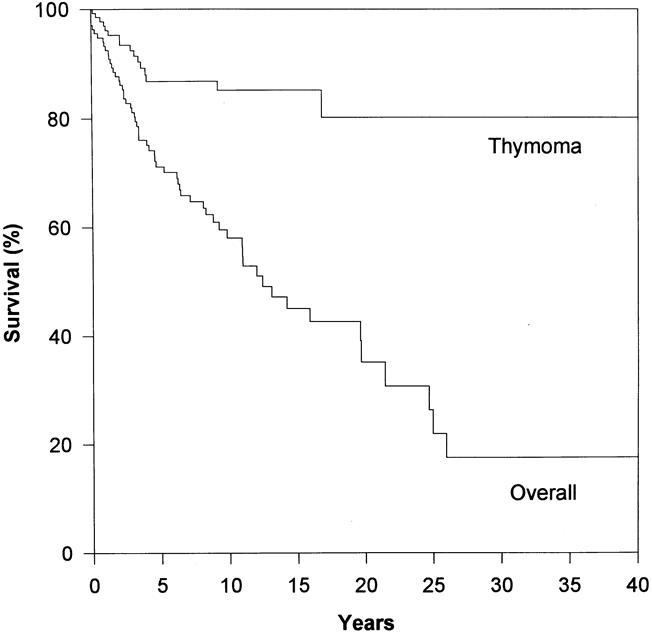
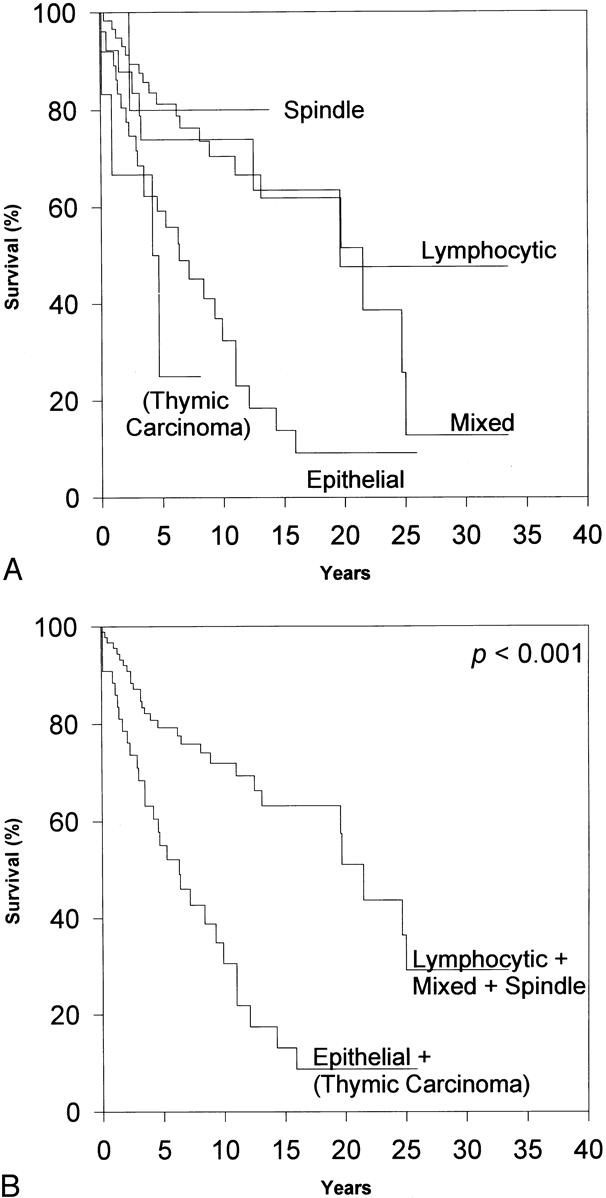
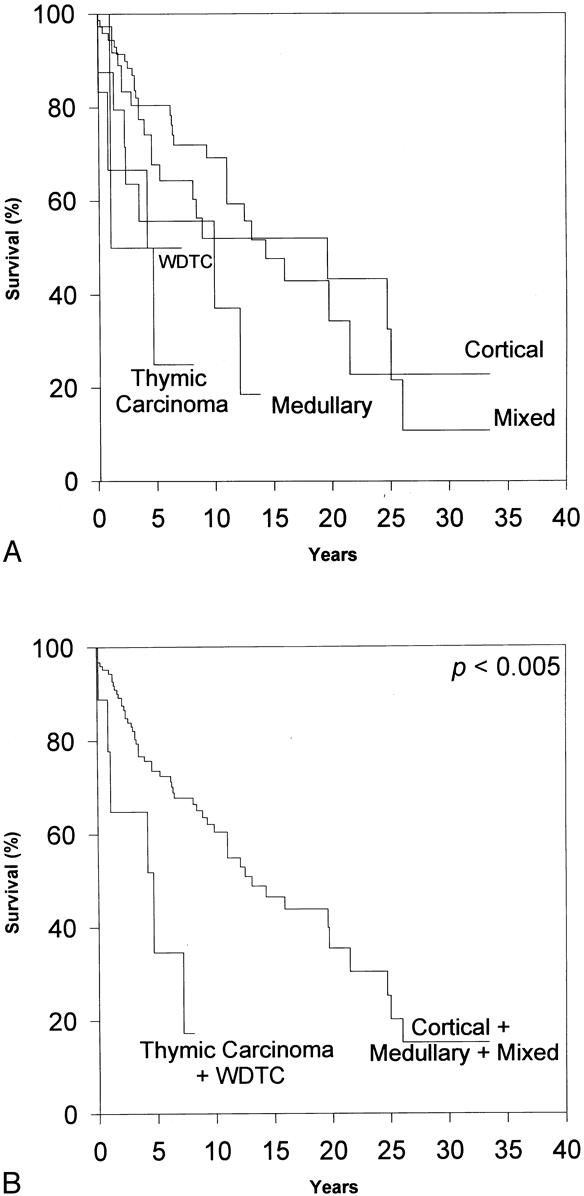
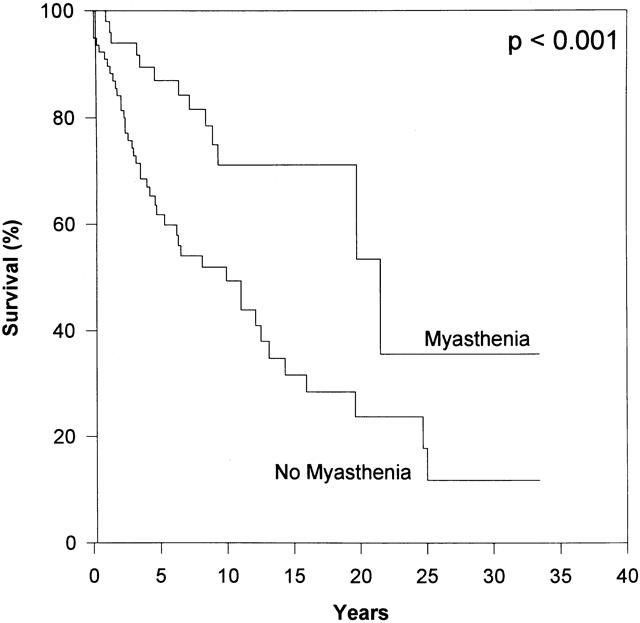
Results: Completeness of follow-up was 99%, 99%, and 98% of eligible patients at 5, 10, and 15 years, respectively. Forty percent of the patients had associated myasthenia gravis and 27% had a secondary primary malignancy. Overall patient survival rates were 71%, 56%, 44%, 38%, and 33% at 5, 10, 15, 20, and 25 years, respectively. Overall, the thymoma-related mortality rate was 14%; the nonthymoma-related mortality rate was 26%. Incomplete resection, preoperative absence of myasthenia gravis, and advanced Lattes/Bernatz pathologic class were found to be independent predictors of poorer overall survival.
Conclusions: These findings support a policy of aggressive, complete surgical resection of all thymomas when feasible. Thymoma behaves as a rather indolent tumor, with most deaths from causes unrelated to thymoma or its direct treatment. Clinicians should have an increased awareness of the possibility of second primary malignancies in patients with thymoma.
Figures
References
-
- Morgenthaler TI, Brown LR, Colby TV, et al. Thymoma. Mayo Clin Proc 1993; 68: 1110–1123. - PubMed
-
- Rosai J, Levine GD. Tumors of the thymus. Washington DC: Armed Forces Institute of Pathology; 1976.
-
- Soudajian JV, Enriquez P, Silverstein MN, Pepin J-M. The spectrum of diseases associated with thymoma. Coincidence or syndrome? Arch Intern Med 1974; 134: 374–379. - PubMed
-
- Verley JM, Hollmann KH. Thymoma. A comparative study of clinical stages, histologic features, and survival in 200 cases. Cancer 1985; 55: 1074–1086. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
