

Long-term functional outcome and quality of life after stapled restorative proctocolectomy
- PMID: 10522727
- PMCID: PMC1420906
- DOI: 10.1097/00000658-199910000-00013
Long-term functional outcome and quality of life after stapled restorative proctocolectomy
Abstract
Objective: To evaluate prospectively long-term quality of life and functional outcome after restorative proctocolectomy (RPC) with ileal pouch-anal anastomosis, and to evaluate and validate a novel quality-of-life indicator in this group of patients.
Summary background data: Restorative proctocolectomy with ileal pouch-anal anastomosis is now the preferred option when total proctocolectomy is required for ulcerative colitis or familial adenomatous polyposis, but long-term data on functional outcome and quality of life after the procedure are lacking.
Methods: Patients (n = 977) who underwent RPC with stapled anastomosis for colitis or polyposis coli and who were followed for > or =12 months were included. Quality of life, fecal incontinence, and satisfaction with surgery were prospectively evaluated by structured interview or questionnaire for 1 to 12 years after surgery (median 5.0). Quality of life was scored using the Cleveland Global Quality of Life (CGQL) instrument (Fazio Score). This is a novel score developed over the past 15 years by the senior author. Quality of life was also evaluated in a subgroup of patients with the Short Form 36 (SF-36). The CGQL was validated by determining its reliability, responsiveness, and validity as well as its correlation with the SF-36 score.
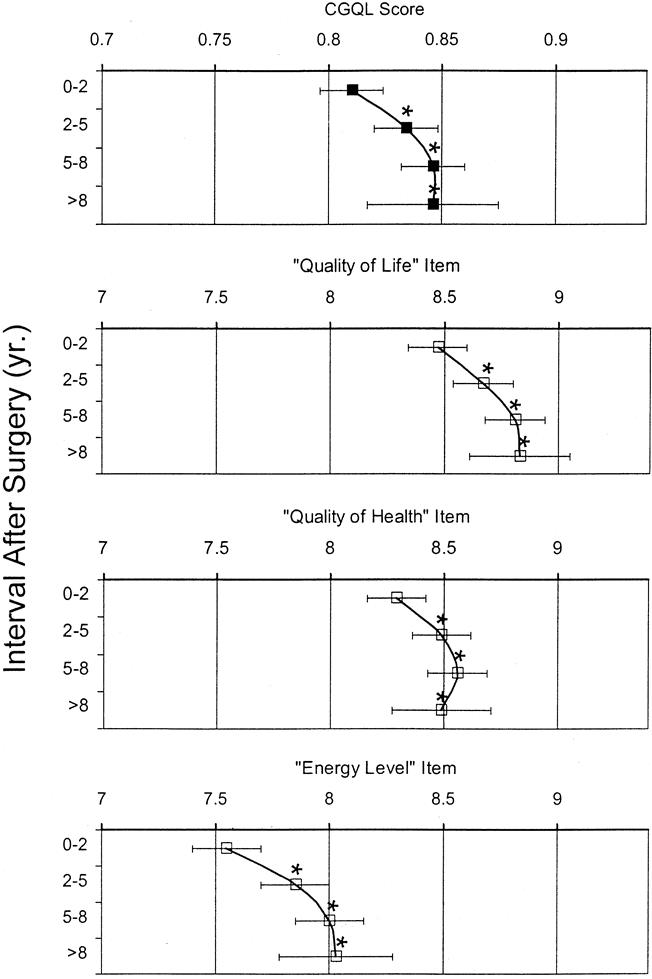
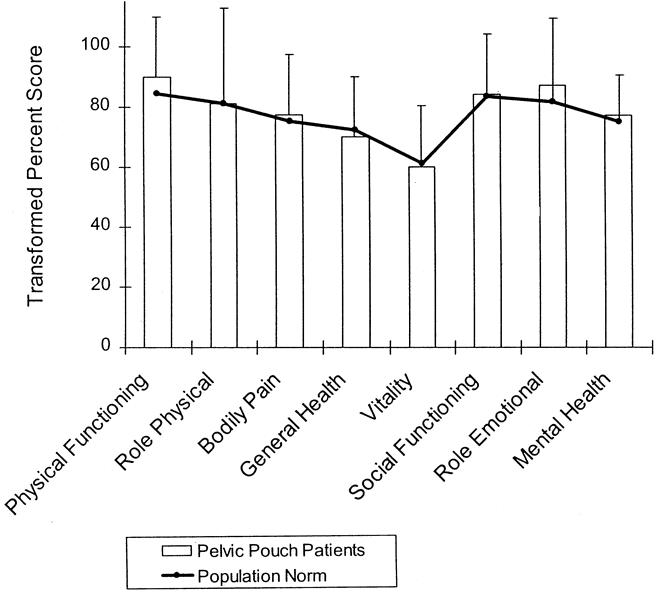
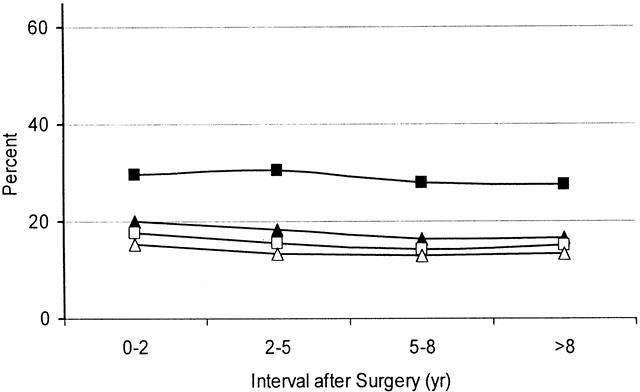
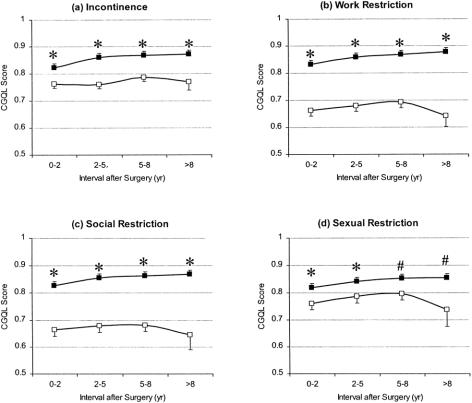
Results: Postoperative quality of life as measured by SF-36 was excellent and compared well with published norms for the general U.S. population. The CGQL was found to be reliable, responsive, and valid, and there was a high correlation with the SF-36 scores. Using the CGQL, quality of life was shown to increase after the first 2 years after surgery, and there was no deterioration thereafter. The prevalence of perfect continence increased from 75.5% before surgery to 82.4% after surgery, and although this deteriorated somewhat >2 years after surgery, it was no worse than preoperative values. Ninety-eight percent of patients would recommend the surgery to others.
Conclusions: Long-term quality of life after ileal pouch surgery is excellent and the level of continence is satisfactory. This surgery is an excellent long-term option in patients requiring total proctocolectomy. The CGQL is a simple, valid, and reliable measure of quality of life after pelvic pouch surgery and may well be applicable in many other clinical conditions.
Figures
References
-
- Fazio VW. Inflammatory bowel disease: surgical aspects. In Farmer RG, Achtar E, Fleshler B., eds. Clinical gastroenterology. New York: Raven Press; 1983: 361–373.
-
- Kelly KA. Anal sphincter-saving operations for chronic ulcerative colitis. Am J Surg 1992; 163: 5–11. - PubMed
-
- Wexner SD, Jensen L, Rothenberger DA, Wong WD, Goldberg SM. Long-term functional analysis of the ileoanal reservoir. Dis Colon Rectum 1989; 32: 275–281. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
