

Clinical Trial
doi: 10.1128/JCM.37.11.3718-3721.1999.
Effects of OspA vaccination on Lyme disease serologic testing
Affiliations
- PMID: 10523583
- PMCID: PMC85737
- DOI: 10.1128/JCM.37.11.3718-3721.1999
Item in Clipboard
Clinical Trial
Effects of OspA vaccination on Lyme disease serologic testing
J Clin Microbiol.
1999 Nov.
Abstract
This study presents the effects of OspA vaccination on two-step testing for Borrelia burgdorferi antibodies. Although vaccinees developed enzyme-linked immunosorbent assay reactivity, immunoblots did not fulfill Centers for Disease Control and Prevention criteria for positivity. Furthermore, OspA reactivity did not interfere with interpretation of immunoblots with sera from patients who developed early Lyme disease despite vaccination.
Figures
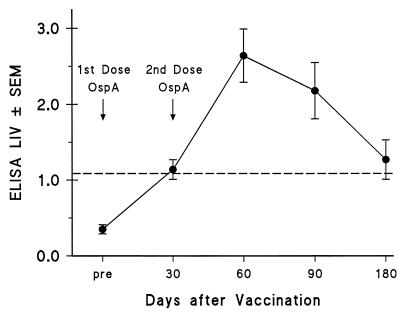
LIVs determined by ELISA (± standard errors of the means) are shown at different times postvaccination in 17 individuals receiving two vaccine doses. The dashed line indicates the cut-off LIV for a positive ELISA (LIV ≥ 1.09). The first vaccination dose was given after collecting the pre serum specimen, and the second dose was administered before the 30-day serum specimen was collected.
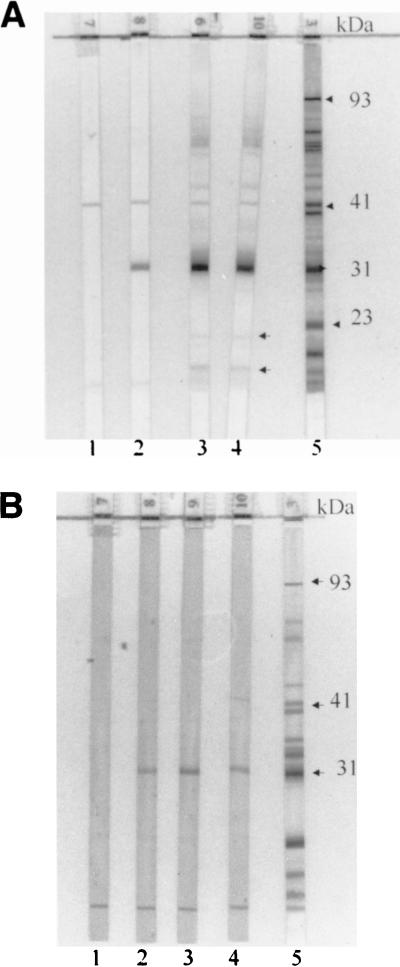
IgG (A) and IgM (B) immunoblot series of serum samples obtained from a vaccinated individual participating in the phase 2 trial at different times postvaccination. Strip numbers are located at the bottom of each strip. Results with pre (strips 1), day 30 (strips 2), day 90 (strips 3), and day 180 (strips 4) samples are shown. Positive controls are shown in strips 5, with arrows indicating a few relevant bands. Those specimens showing the most intense reactivity to OspA in IgG blots (strips 3 and 4) also show reactivity to two other bands below 23 kDa (OspC) (arrows positioned next to strip 4) and diffuse darkening in the upper region of the blot. IgM reactivity to OspA was less intense than IgG reactivity.
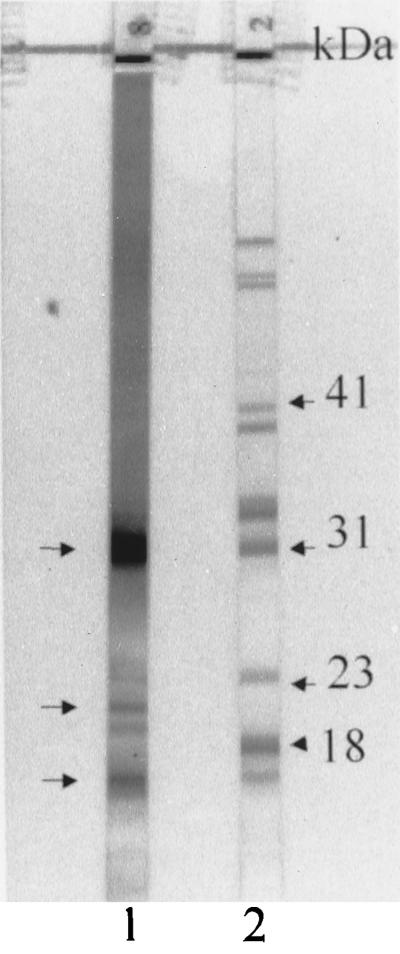
IgG immunoblot of serum samples from an individual who received the third dose of the recombinant OspA vaccine preparation 2 weeks prior to collection of this serum specimen (strip 1). Besides the band of strong reactivity to OspA (top left arrow), two other bands below 23 kDa are visible (bottom two left arrows). These two bands are located above and below the 18-kDa band, which is included in the diagnostic criteria for IgG immunoblot interpretation (3). In addition, there is a general darkening of the immunoblot extending from the superior portion to beyond the 31-kDa band. Strip 2 shows a positive control, with arrows indicating a few relevant bands.
Representative IgG and IgM immunoblots of serum samples from two individuals who received three doses of the OspA vaccine preparation. Strip numbers are shown at the bottom of each strip. Strip 1 shows a positive control, and the arrows on the left indicate a few relevant bands. Strips 2 and 3 show the IgG and IgM immunoblots, respectively, of a serum sample from one individual collected 6 weeks after the third dose of vaccine. Strips 4 and 5 show the IgG and IgM reactivities of a serum sample collected from another individual 5 weeks following the third vaccine dose.

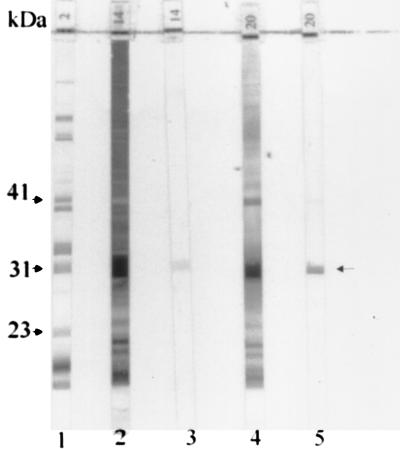
IgM and IgG blots of serial serum specimens from two patients who developed early Lyme disease associated with erythema migrans despite OspA vaccination. Strip numbers are shown at the bottom of each strip. (A) IgM (strips 1 to 4) and IgG immunoblots (strips 6 to 9) of serum samples from a patient who presented with erythema migrans (confirmed by a positive culture for B. burgdorferi) 6 months after the second vaccine dose. Serum specimens were collected prior to the first vaccine dose (strips 1 and 6) and 1 day (strips 2 and 7), 8 days (strips 3 and 8), and 3 weeks (strips 4 and 9) after onset of erythema migrans. A positive control is shown in strip 5, with arrows indicating a few relevant bands. The IgG immunoblots postvaccination show weak reactivity to OspA, and new IgG bands were observed in the acute- and convalescent-phase specimens. IgM immunoblots showed the appearance of the 41- and 23-kDa bands in the specimen collected 8 days postonset of illness, with expansion of reactivity at 3 weeks. (B) IgM (strips 1 to 3) and IgG (strips 5 to 7) immunoblot series of serum samples from a patient presenting with a 2-day history of multiple erythema migrans lesions when the serum specimens shown in strips 3 and 7 were collected. Strips 1 and 5 show the IgM and IgG immunoblots, respectively, of serum specimens collected prior to the first vaccine dose, and strips 2 and 6 show the IgM and IgG immunoblots of serum specimens collected prior to the third vaccine dose. The serum specimens shown in strips 3 and 7 were obtained 12 days after the third vaccine dose. Strip 4 shows a positive control, with arrows indicating a few relevant bands. Note that the IgM bands of diagnostic significance were not affected by the presence of IgM reactivity to OspA (strip 3). Strip 7 shows intense IgG reactivity to OspA and a general darkening of the immunoblot. Arrows located to the right of strip 7 indicate the frequently observed bands after two to three doses of vaccine, at 31 kDa and two bands below OspC.
References
-
- American College of Physicians. Guidelines for the laboratory evaluation in the diagnosis of Lyme disease. Ann Intern Med. 1997;127:1106–1108. - PubMed
-
- Anonymous. Lyme disease vaccine approved. JAMA. 1999;281:405.
-
- Centers for Disease Control and Prevention. Recommendations for test performance and interpretation from the Second National Conference on Serologic Diagnosis of Lyme Disease. Morbid Mortal Weekly Rep. 1995;44:590–591. - PubMed
-
- Johnson B J B, Robbins K E, Bailey R E, Cao B-L, Sviat S L, Craven R B, Mayer L W, Dennis D T. Serodiagnosis of Lyme disease: accuracy of a two-step approach using a flagella-based ELISA and immunoblotting. J Infect Dis. 1996;174:346–353. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
