

Disseminated aspergillosis involving the brain: distribution and imaging characteristics
- PMID: 10543627
- PMCID: PMC7056178
Disseminated aspergillosis involving the brain: distribution and imaging characteristics
Abstract
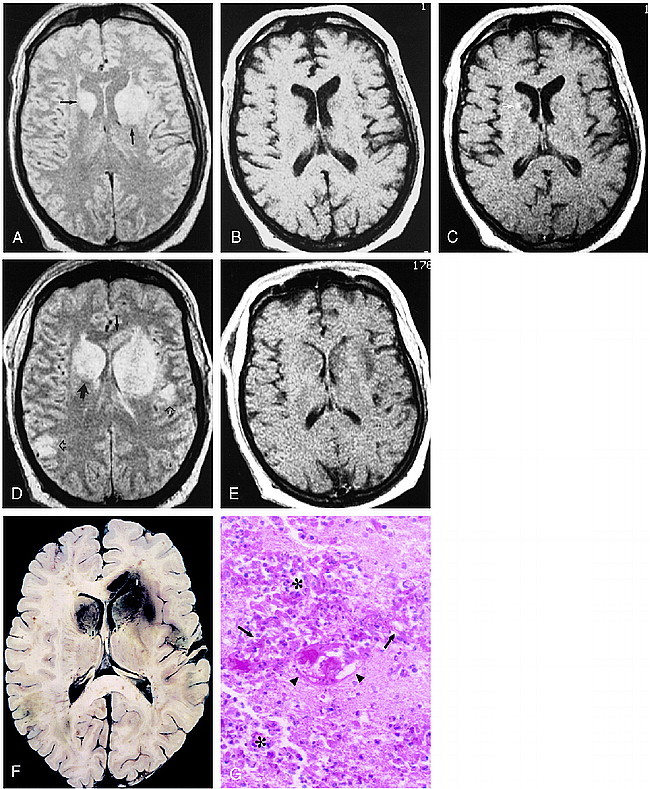
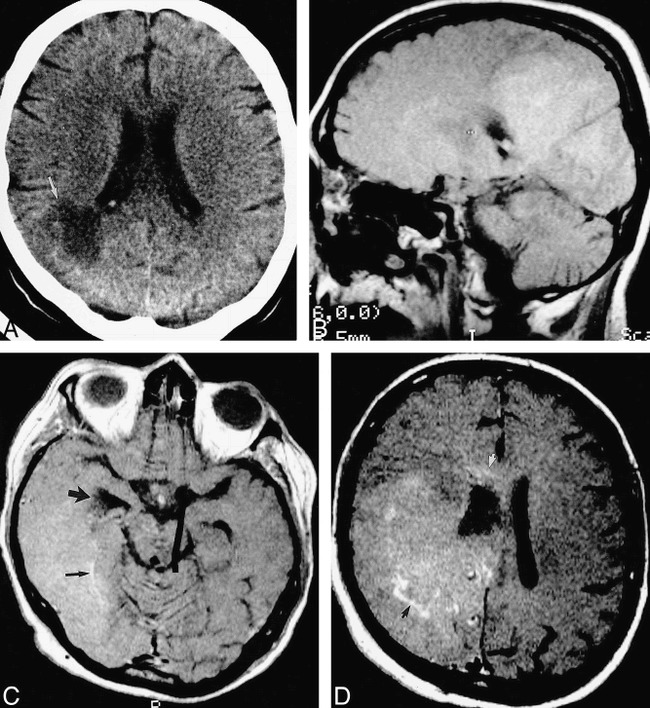
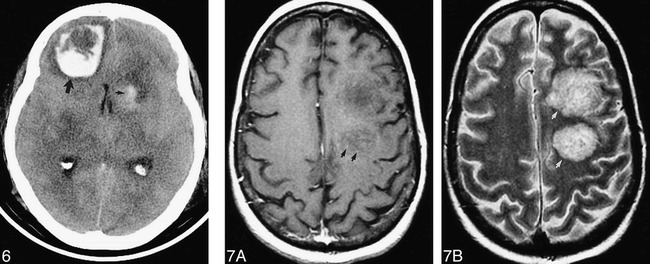
Background and purpose: Systemic invasive aspergillosis involves the brain through hematogenous dissemination. A retrospective review of 18 patients with aspergillosis involving the brain was performed in order to present imaging findings and thereby broaden the understanding of the distribution and imaging characteristics of brain Aspergillus infection and to facilitate its early diagnosis.
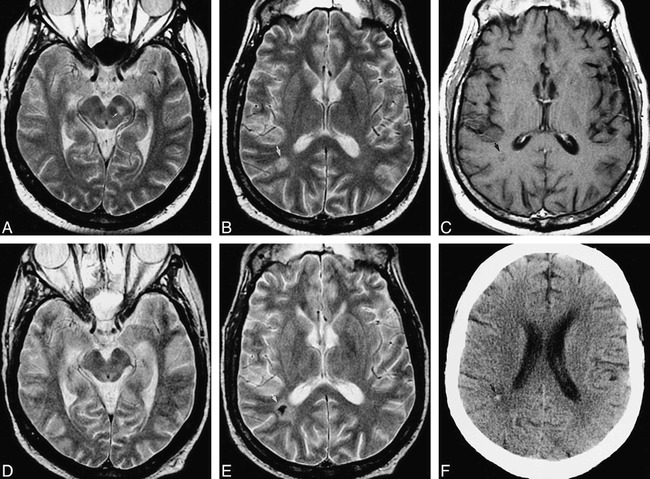
Methods: The neuroimaging studies of 17 biopsy- or autopsy-proved cases and one clinically diagnosed case were examined retrospectively by two neuroradiologists. The studies were evaluated for anatomic distribution of lesions, signal characteristics of lesions, enhancement, hemorrhage, and progression on serial studies (when performed). Medical records, biopsy reports, and autopsy findings were reviewed.
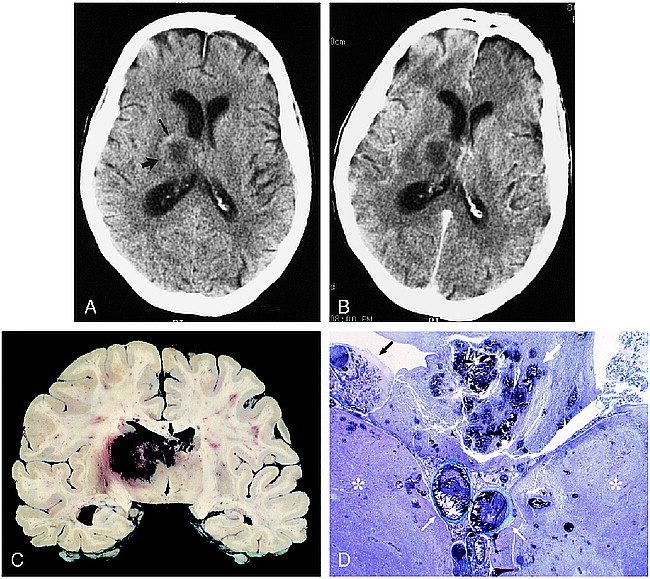
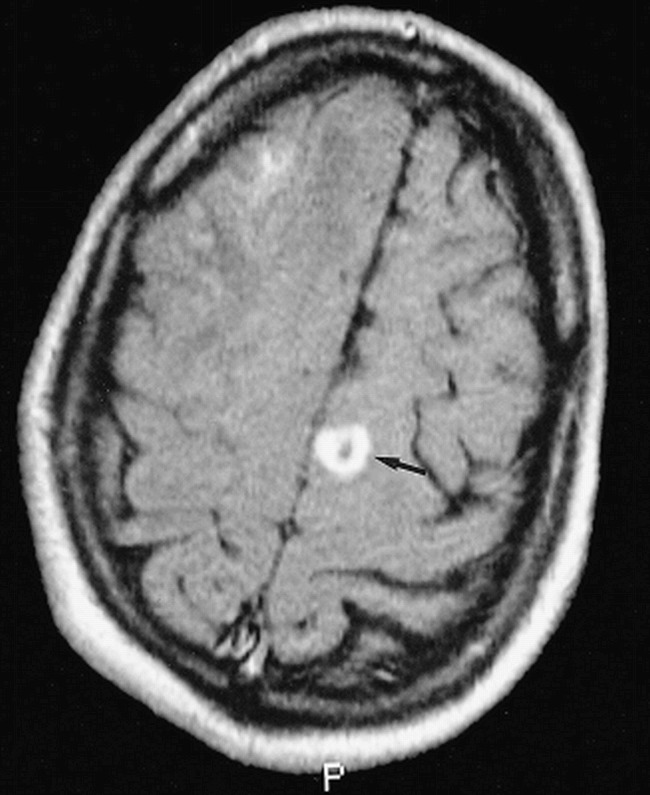
Results: Thirteen of 18 patients had involvement of the basal nuclei and/or thalami. Nine of the 10 patients with lesions at the corticomedullary junction also had lesions in the basal nuclei or thalami. Callosal lesions were seen in seven patients. Progression of lesion number and size was seen in all 11 patients in whom serial studies had been performed. Enhancement was minimal or absent in most cases. There was gross hemorrhage in eight of the 18, and definite ring-enhancement in three.
Conclusion: Among our cases, lesions in perforating artery territories were more common than those at the corticomedullary junction. Ring enhancement and gross hemorrhage may be present, but are not necessary for the prospective diagnosis.
Figures
References
-
- Pagano L, Ricci P, Montillo M, et al. Localization of aspergillosis to the central nervous system among patients with acute leukemia: report of 14 cases. Gruppo Italiano Malattie Ematologiche dell'Adulto Infection Program. Clin Infect Dis 1996;23:628-630 - PubMed
-
- Khoury H, Adkins D, Miller G, Goodnaugh L, Brown R, DiPerso J. Resolution of invasive central nervous system aspergillosis in a transplant recipient. Bone Marrow Transplant 1997;20:179-180 - PubMed
-
- Schwartz S, Milatovic D, Thiel E. Successful treatment of cerebral aspergillosis with a novel triazole (voriconazole) in a patient with acute leukemia. Br J Haematol 1997;97:663-665 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical